COMPLEX NUCHAL MASS |
|
Assess upper cervical spine and occiput ß ß ß ß ß ß ß ß ß ß |
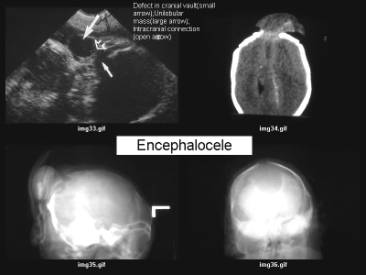
Þ Bony defect |
Encephalocele or
|
|
|
|
|
ß ß |
|
|
|
|
|
|
Exclude ß ß ß ß ß Cystic Hygroma |
|
|
|
||





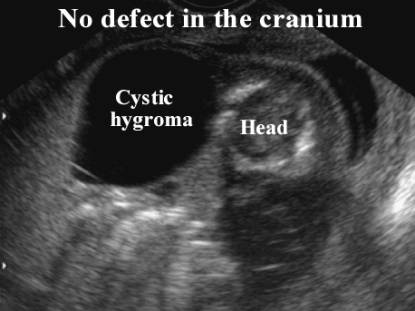
NUCHAL CYSTIC HYGROMA |
Cystic hygromas are congenital malformations of the lymphatic system, and are characterized by single or multiple fluid filled lesions that occur at sites of lymphatic-venous connection. Once considered diagnostic of Turner’s syndrome, they are now known to be associated with other karyotypic abnormalities and several malformation syndromes (1-6).
ULTRASOUND OF HYGROMA IN THE FIRST TRIMESTER |
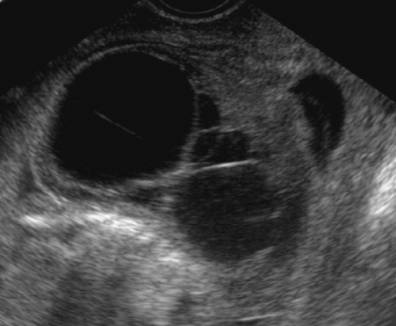
1. Earliest sign is increased nuchal translucency. The degree of cystic changes is not as well developed, and septations are less likely.
2. Chromosomal abnormalities are present in 50% (usually autosomal trisomy). See section on Nuchal translucency screening.
3. If no chromosomal abnormality is present and no other sonographically detectable anomaly is present, the prognosis appears good. They are usually small, unilocular and unilateral, and often resolve with a normal postnatal appearance (7). It is thought to be due to a delay in the jugulo-lymphatic connection that results in transient fluid in the neck that resolves once the connection is established.
Cystic
hygromas between 9-14 weeks
|
|
|
Chromosomal
abnormalities (29%) |
No chromosomal
abnormalities (71%) |
|
Trisomy 18 (38%) |
Adverse outcome (30%) |
|
Trisomy 21 (31%) |
|
|
Turners syndrome (XO) (25%) |
|
|
47,XXX (6%) |
|
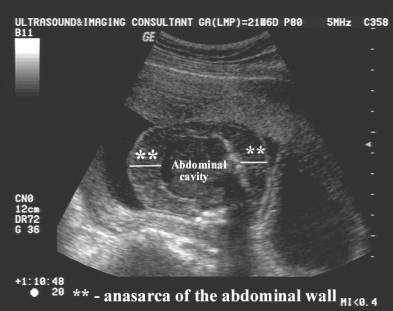
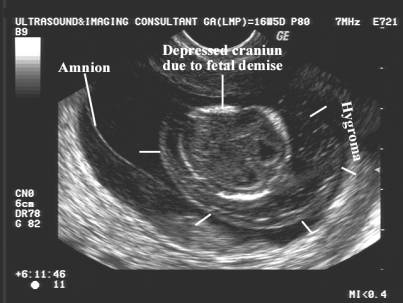
ULTRASOUND OF HYGROMA IN THE SECOND TRIMESTER |
|
Lesions that persist into the
second trimester or lesions that are discovered in the second trimester are
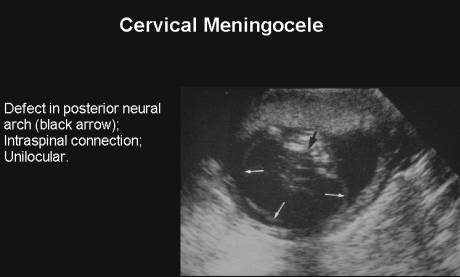
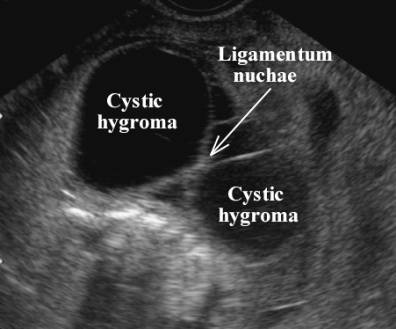
associated with a poorer prognosis (1-5). 1. Midline cervical mass with midline septum (ligamentum
nuchae).
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3D Cystic hygroma |
|
|
|
|
|
Cystic hygromata associated with a normal karyotype may have a wide range of inherited disorders and
malformation syndromes (9).
The risk of a second malformation is estimated at 30% - persistent left superior vena cava, intestinal malrotation, duodenal atresia and imperforate anus (10). |
|
|
Cystic hygromata have been associated with teratogen
exposure including alcohol, aminopterin and
trimethadione (5). |
|











Chromosomal anomalies in 900 karyotyped fetuses with
cystic hygroma (8)
|
|||
|
Chromosomal Anomaly |
All
fetuses |
First Trimester |
Second Trimester |
|
Turner’s
syndrome (XO) |
31.3% |
12.1% |
42.7% |
|
Trisomy
21 |
15% |
21.4% |
11.3% |
|
Trisomy
18 |
7.3% |
13.7% |
3.5% |
|
Trisomy
13 |
2.5% |
3% |
2.3% |
|
Other
abnormal karyotypes |
3.9% |
4.8% |
3.4% |
|
Normal |
40% |
45% |
36.8% |
Comparison of “non-septated “ cystic spaces
and septated cystic hygroma
|
||
|
|
“Nonseptated” cystic space” |
Cystic hygroma |
More likely to persist |
2% |
56% |
|
Aneuploidy |
5.6% |
72% |
|
Hydrops |
1.7% |
40% |
|
Associated anomalies |
15% |
52% |
|
Pregnancy loss |
6% |
88% |
REFERENCES |
- MacLeod AM, McHugo JM. Prenatal Diagnosis of Nuchal Cystic Hygroma. Br J Radiol 1991; 64:802-807
- Bronshtein M, Bar-Hava I, Blumenfeld I et.al. The difference between Septated and Nonseptated Nuchal Cystic Hygroma in the early Second Trimester Obstetrics and Gynecology 1993; 81:683-687
- Suchet IB, van der Westhuizen NG, Labatte MF. Fetal cystic hygromas: further insights into their natural history. Can Assoc Radiol J 1992; 43:420-424
- Cullen MT, Gabrielli S, Green JJ et.al. Diagnosis and significance of cystic hygroma in the first trimester. Prenat Diagn 1990; 10:643-651
- Edwards MJ, Graham JM. Posterior Nuchal Cystic Hygroma. Clinics in Perinatology 1990; 17:611-640
- Chitayat D, Kalousek DK, Bamforth JS. Lymphatic abnormalities in fetuses with posterior cervical cystic hygroma. Am J Med Gen 1989; 33:352-356
- Bernstein HS, Filly RA, Goldberg JD et.al. Prognosis of fetuses with cystic hygromata. Prenat Diagn 1991;11:349-355
- Machin G. Hydrops, cystic hygroma, hydrothorax, pericardial effusion and fetal ascites. In: Gilbert Barness E (ed): Potters pathology of the fetus and infant. Mosby, St Louis 1997;pg 163-181
- Gallagher PG, Mahoney MJ, Gosche JR. Cystic hygroma in the fetus and newborn. Sem Perinatol 1999;23(4):341-356
- Geifman-Holtzman O, Drury
HE, Holmes LB. Increased detection of cystic hygroma: A
“technology-induced” phenomenon. Teratology 1996;54:298-302