|
CLOACAL
MALFORMATION CLOACAL DYSGENESIS SEQUENCE
|
Definition: Association of an imperforate anus with confluence of the rectum, vagina, and bladder in a urogenital sinus.
Cloaca = sewer in Latin.
Synonyms: Anorectal anomalies, persistent cloaca, cloacal malformations.
Incidence: Cloacal malformations occur in approximately 0.2:10,000 live female births. The incidence in male is not well established which may result from an ascertainment bias.
Etiology: Sporadic. Rare cases have been associated with chromosomal anomalies. In the mouse, a similar type of anomalies occur with mutations of the Hoxa-13 and Hoxd-13 and Etretinate, a synthetic retinoid can cause similar anomalies.
EMBRYOLOGY |
3- to 5-week-old embryo:
- The urinary, genital and distal gastrointestinal tracts empty into a common channel called the cloaca in the (63).
- The confluence of the allantois and the hindgut in this common chamber is a widely accepted stage in embryonic development.
- The cloaca is covered by a membrane that occupies the space between the tail and the body stalk and is not opened externally at this stage of development (64).
By the 6th gestational week:
- The cloaca is segregated into an anterior urogenital sinus and a posterior intestinal canal by the cranial-to-caudal descent of the urorectal septum.
- This descent is accompanied by migration of the lateral folds of the cloaca toward the midline.
- The urorectal septum, a wedge of mesoderm, normally extends to the cloacal membrane by the 7th week.
- The caudal extension of the urorectal septum develops into the perineal body, dividing the perineum into the urogenital triangle ventrally and the anal triangle dorsally.
o In the male, the inner and outer genital ridges fuse to form the anterior urethra.
o In the female, these ridges do not coalesce, and so develop into the labia minora and majora.
- The urogenital sinus is divided into three parts:
o a cranial vesical part that is continuous with the allantois,
o a middle pelvic part,
o and a caudal phallic part that is closed externally by the urogenital membrane (4, 64).
- Arrest of division of the cloaca by the urorectal septum at varied times between the 4th and 12th weeks of gestation leads to the wide spectrum of anorectal malformations. The intimate association of the embryologic development of the anorectal, genital, and urinary systems also explains the frequency with which simultaneous associated malformation in these systems are encountered (65).
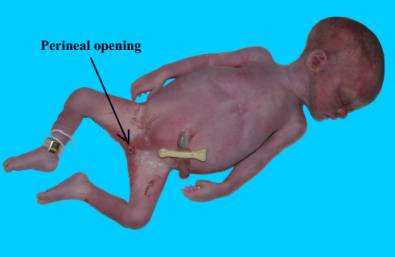
Cloacal malformation represents persistence of an early embryonic state in which the urinary, genital and gastrointestinal tracts all drain through a common perineal opening. This anomaly is believed to result from failure of the urorectal septum to join the cloacal membrane during the 4th to 6th week of embryonic life (52). This rare anomaly occurs only in phenotypic girls (66). The perineum of the typical patient has a single opening that serves as the outlet for urine, genital secretions, and feces or meconium, and the abdominal wall is normal (67).
ULTRASOUND |
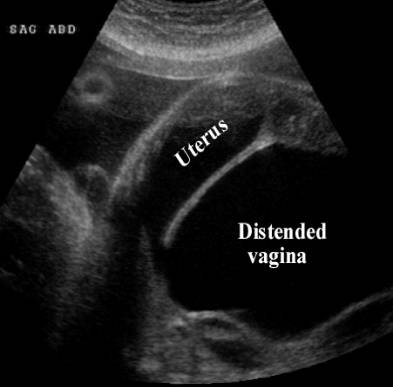
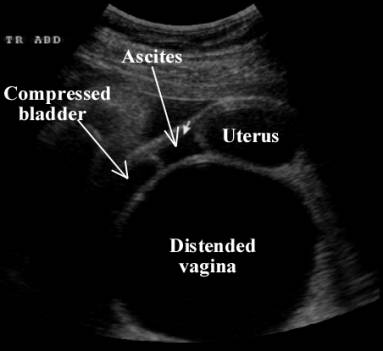
The typical appearance is that of a pelvic fluid-filled structure, whose appearance depends on the anatomy involved and the gestational age. In the first trimester, the main finding may be dilated loops of bowel, then megacystis, ascites and oligo/anhydramnios occurs when no external opening is present. The perineum is smooth with absence of anal, urethral, and/or vaginal openings. The labia majora and minora may be absent in females and the scrotum and penis may be absent or hypoplastic in males.
|
Distended
vagina and uterus |
|
|
|
|
|
|
|
|
|
|
|
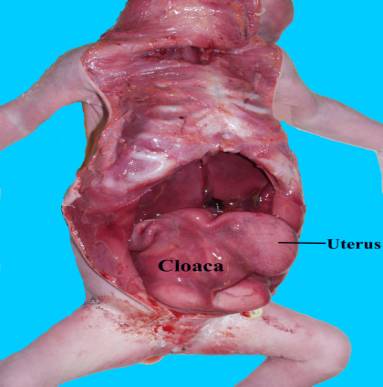
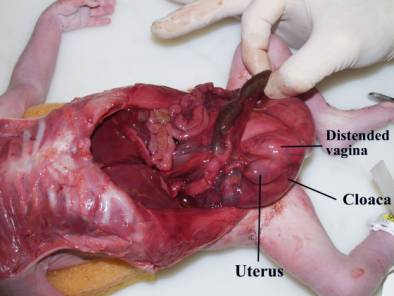
Absent anal
opening |
|
|
|
|
|
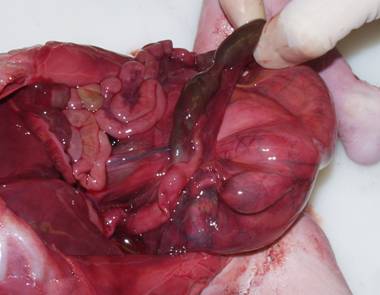
Bowel loop draining into cloaca (note green meconium in
bowel). Small arrow on ultrasound images delinates intraluminal calcified meconium
(enterolithiasis). |
|


DIFFERENTIAL DIAGNOSIS |
Obstructive uropathy, but a large bladder should be visible and Vacterl.
ASSOCIATED ANOMALIES |
Cardiac, pulmonary (hypoplastic lungs), renal (renal agenesis, dysplasia, hydronephrosis, hydroureters), gastrointestinal (intraluminal colonic calcifications) skeletal and vertebral anomaliesg rowth restriction, single umbilical artery.
PROGNOSIS |
In cases with no outlet of the urine into the amniotic cavity, the prognosis is fatal due to lung hypoplasia, but there are exceptions. Among those surviving to surgery, in a large series of 141 patients:
Ø 82 have spontaneous bowel movements and satisfactory control,
Ø 38 use enemas to evacuate,
Ø 9 have a colostomy,
Ø 7 have fecal soiling, and
Ø 5 are too recently operated to evaluate.
REFERENCES |