|
MULTILOCULAR CYSTIC
NEPHROMA |
ULTRASOUND |
- A discrete multiseptated cystic mass that primarily involves the kidney.
- Very rare in the fetus.
CT
features include:
·
a
well-marginated, rounded, or polycyclic cortical mass that extends beyond the
normal renal outline.
·
This
mass contains cysts that vary in size and number. It may be a cluster of a few
large cysts with thick walls and septa, or it may be a denser mass composed of
tiny cysts.
·
Enhancement
of the septae may be seen due to the presence of thin vessels in the septae.
MRI
features include:
·
A
solitary cystic lesion with thin internal septations or a cluster of closely
grouped cysts of similar size. Individual cystic spaces demonstrate varying
signal intensity.
·
A
complex cystic renal lesion with enhancing septa and herniation into the renal
collecting system are the characteristic MR findings.
·
The
direct multiplanar capability of MR may optimally show the relationship to the
renal pelvis and thus facilitate correct diagnosis.
·
The
locules will not fill in with contrast on CT, MRI or intravenous urography.
·
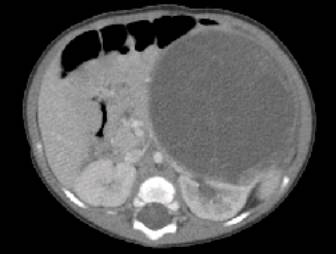
Hydronephrosis is often present in the
remainder of the kidney secondary to compression by the large mass. A careful
evaluation should be made for any areas of marked septal nodularity or discrete
solid components. If these lesions are identified, then suspicion should be
raised that this could be a cystic Wilms' tumour or possibly Wilms' tumour
coexisting with CPDN.
Postnatal renal ultrasound
|
|
|
|
|
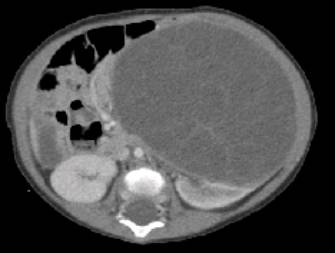
Postnatal enhanced CT scan
|
|
|
|
|


DIFFERENTIAL DIAGNOSIS |
Radiographic
differential diagnosis includes Wilms tumour with cyst formation due to
haemorrhage and necrosis, cystic clear cell sarcoma (see clear cell sarcoma
renal), cystic renal cell carcinoma, and multicystic dysplastic kidney.
Multilocular cystic renal tumor is a term that encompasses two histologically distinct but grossly indistinguishable lesions: cystic nephroma and cystic partially differentiated nephroblastoma (CPDN). Cystic nephroma is a segmental, purely cystic mass characterized by multiple septations composed entirely of differentiated tissues, without blastemal elements. CPDN is also a multiloculated lesion without nodular solid components, but its septa contain embryonal cells. Multilocular cystic tumors primarily affect boys during early childhood, with a substantial number of the lesions containing blastema (CPDN), and adult women, with lesions that more commonly lack septal blastema (cystic nephroma). As a rule, nephrectomy is curative and the clinical course benign, but CPDN may recur locally. Although cystic nephroma and CPDN cannot be distinguished radiologically, failure to do so has no practical impact on management, since all of these tumors are surgically removed. However, the differential diagnosis includes other pediatric cystic renal masses that may require different treatment
Imaging
cannot distinguish between cystic nephroma and CPDN.
·
Both
tumours are well encapsulated and often large.
·
They
are unilateral and involve only one part of the kidney.
·
Often
they are located close to the renal pelvis, and herniation of the renal pelvis
is a pathognomonic finding on intravenous urography, CT or MRI.
They contain multiple non-communicating cysts with thin septa separating the cysts. Cyst fluid can either be clear or straw-colored or a thick gelatinous substance.
Treatment of multilocular cystic renal tumour is surgical. The tumours are benign. However, in certain cases of CPDN, local recurrence can occur following surgical resection. Prognosis is excellent stratagems: Wilms tumor with cyst formation due to hemorrhage and necrosis, cystic clear cell sarcoma, cystic mesoblastic nephroma, cystic renal cell carcinoma, multicystic dysplastic kidney, and segmental multicystic dysplasia in a duplicated renal collecting system.
REFERENCES |
1. Alanen A, Nurm M, Ekfors T. Multilocular renal
lesions: a diagnostic challenge. Clin Radiol 1987; 38: 475-477.
2. Hartman
DS, Davis CJ, Sanders RC et al. The multiloculated renal mass:
considerations and differential features. Radiographics1987; 7: 29-52.
3. Madewell
JE, Goldman SM, Davis CJ et al. Multilocular cystic nephroma: a
radiologic-pathologic correlation of 58 patients. Radiology 1983; 146: