|
PELVIC KIDNEY |
Renal ectopia is defined as malposition
of the kidney(s) due to faulty migration from the fetal pelvis during early
embryologic development.
EMBRYOLOGY |
The kidneys migrate to the renal fossa by passing through the arterial fork created by the umbilical arteries in early embryological development. If one or both kidneys fail to migrate, they remain in the pelvis close to the common iliac artery. The process of renal ascent occurs during the 10th week of gestation (1). The adrenal gland has an entirely different embryonic derivation (the medulla is of neural crest ectodermal origin and the cortex is mesodermal). This explains the normal position of the adrenal glands in renal agenesis or ectopia. As the kidney ascends the blood supply changes; the lower vessels atrophy with a more cephalad origin develop. The renal arteries initially develop from the iliac artery and then from higher sights of the aorta sequentially as the kidneys ascend.
If the normal ascent to the renal fossa is incomplete, the kidney may remain
in the pelvis or anywhere between the bony pelvis and renal fossa.
ULTRASOUND |
- May be unilateral or rarely bilateral (2,3).
- Localized below the aortic bifurcation (unlike a lumbar kidney which lies anterior to the iliac vessels).
- Size of the ectopic kidney is usually normal.
- The bladder is normal.
- The adrenal glands are in their normal position.
- Blood supply from the middle sacral artery or iliac artery.
|
|
|
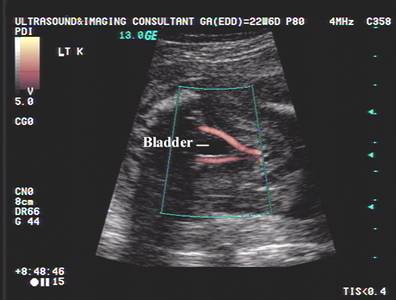
Antenatal scan at 23 wks gestation
|
|
|
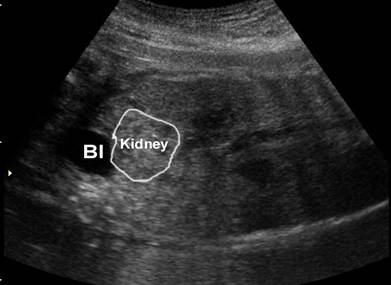
32 weeks of gestation – note the blood supply to the pelvic
kidney is from the right common iliac artery |
|
|
|
|
|
|
|
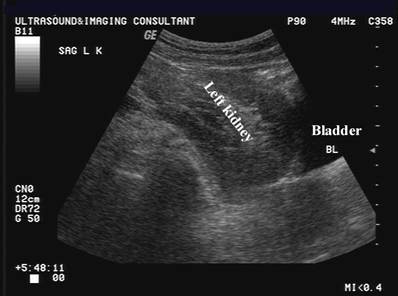
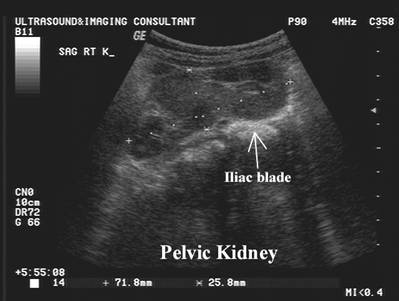
Postnatal ultrasound –
Left pelvic kidney
|
|
|
|
|
|
|
|







DIFFERENTIAL DIAGNOSIS |
- Unilateral renal agenesis.
- Crossed fused renal ectopia.
ASSOCIATED ANOMALIES (4,5) |
- The contralateral kidney may be congenitally absent or anomalous (3).
- Skeletal anomalies.
- Genitourinary anomalies.
- Cardiovascular anomalies.
- Anomalies of the female reproductive system.
COMPLICATIONS |
- Increased frequency of hydronephrosis, malrotations and impaired urinary drainage.
- Obstruction of an upper pole calyx or ureter has been reported (6).
REFERENCES |
- Meizner I, Yitzhak M, Levi A et.al. Fetal pelvic kidney: a challenge in prenatal diagnosis? Ultrasound Obstet Gynecol 1995; :391-393.
- Meizner I, Barnhard Y. Bilateral fetal pelvic kidney: Documentation of two cases of a rare prenatal finding. J Ultrasound Med 1995;14:487-489.
- Melek R, Kelalis PP, Burke EC. Ectopic kidney in children and frequency of association with other malformations. Mayo Clin Proc 1971;46:461-467.
- D'Alberton A. Prevalence of urinary tract abnormalities in a large series of patients with ureterovaginal atresia. J Urol 1981;126:623.
- King KL, Kofinas AD, Simon NV et.al. Prenatal diagnosis of fetal pelvic kidney. J Reprod Med 1993;38:225-226.