|
FETAL
EXTRASYSTOLES |
- Fetal extrasystoles are the most common fetal arrhythmia that results in an irregular fetal heart rate (early or premature beat).
- Benign and usually self-limiting and do not generally compromise cardiac function.
- Extrasystoles usually last < 750 msec.
- Premature atrial contractions are more common than those of ventricular or junctional origin (however differentiation between the three types may be difficult and often impossible).
- Patients should be counseled to avoid stimulating drugs like caffeine, cocaine, adrenergic drugs (pseudoephedrine) and beta-mimetic tocolytics.
- Two main types: Atrial PAC (more frequent and has a P wave). Ventricular PAC (no P wave).
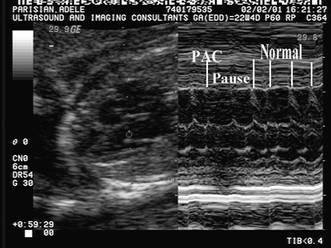
ULTRASOUND OF PREMATURE ATRIAL CONTRACTION (PAC) |
- Either conducted or non conducted and occurs in about 1-2% of pregnancies.
- They are usually benign and resolve spontaneously.
- 1-2% are associated with structural cardiac defects (most commonly Ebstein’s, tricuspid valve dysplasia and cardiac tumors).
- 1% risk for the development of supraventricular tachycardia.
- Non-conducted:
No aortic flow following the premature atrial systole when sampling the normal aortic outflow tract. Following the PAC there is a pause. The next beat is a sinus beat with normal atrial and ventricular contraction - Conducted:
Aortic flow can be demonstrated following premature atrial systole. Following the PAC there is ventricular contraction then a pause prior to the resumption of sinus rhythm.
|
|
|

|
M-mode
echocardiography |
Premature movement of the posterior atrial wall. |
||
|
|
|
||
|
Doppler studies |
Passive E wave filling of the ventricle during ventricular
systole. |
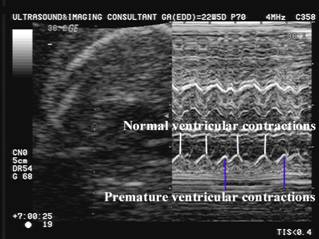
ULTRASOUND OF PREMATURE VENTRICULAR CONTRACTION |
- Usually resolve spontaneously prior to delivery.
- Those that persist into neonatal period usually resolve within 6 weeks.
- Rarely results in more complex arrhythmias (supraventricular tachycardia in 0.4-1% of cases). Fetuses should therefore be scanned once or twice weekly.
- Can be associated with:
- Myocarditis (cardiomyopathy).
- Cardiac tumors (rhabdomyomas)
- Long QT syndrome.
- Complete AV block with slow ventricular escape rhythm.
|
M-mode echocardiography |
Place cursor through atrial and ventricular wall to observe the mechanical results of the electrical event. |
||
|
|
|
||
|
Doppler studies |
|

COMPLICATIONS |
There is a 0.5% risk of supraventricular
tachycardia (SVT) developing in fetuses with premature atrial
extrasystole. One-week follow up is recommended to
reduce the risk of the fetus developing non-immune hydrops
from sustained SVT.
REFERENCES |
- Copel JA, Friedman AH, Kleinman CS. Management of fetal cardiac arrhythmias. Obstet Gynecol Clin North Am 1997;24:201-211.