|
ANEURYSM OF THE
DUCTUS ARTERIOSUS |
Most of the previous reported cases of ductus arteriosus aneurysm were noted incidentally at neonatal
autopsy, and are thought to be due to transient widening of the ductus prior to spontaneous obliteration and not due to
true aneurysms (1-3).
|
ETIOLOGY |
There are several proposed theories. Some workers (1) believe that delayed closure of the aortic end may result in exposure of the weakened ductal wall to systemic pressure which may lead to aneurysm formation. This view is supported by the observation that in all reported cases of neonatal ductus arteriosus aneurysm, the aortic end was open but only 30% were patent at the pulmonary end (1). Another theory suggests congenital or acquired weakening of the ductus wall (4). A third theory has been proposed (2) which suggests that increased blood flow through the ductus (both their cases were associated with arteriovenous shunts- vein of Galen AVM and hepatic angioma).
Additional suggested etiologies include:
- Connective tissue disorders (Marfan's, Ehlers-Danlos and Larsen syndrome)
- Infection (1,5).
|
ULTRASOUND |
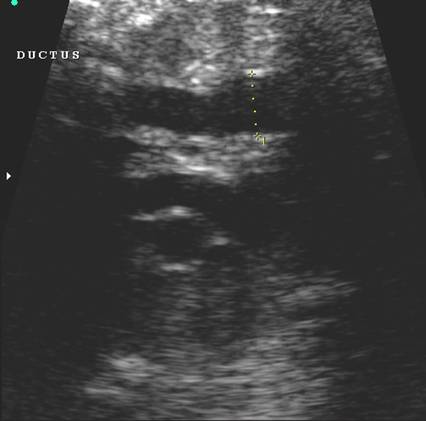
- Normal ductus arteriosus
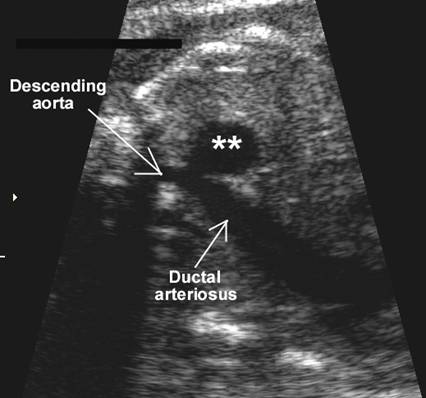
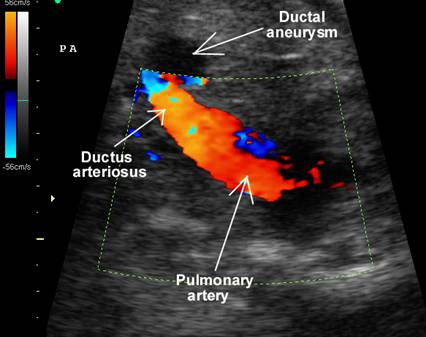
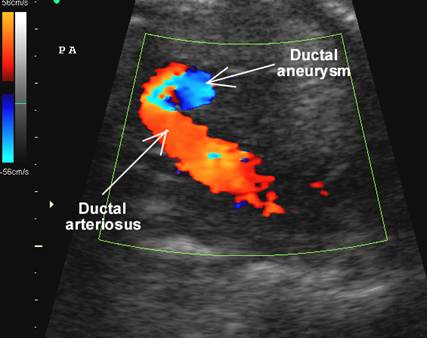
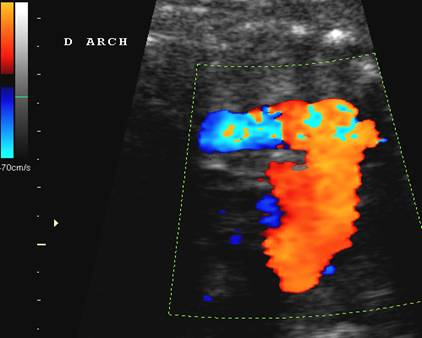
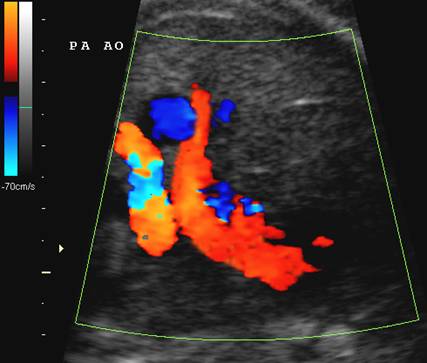
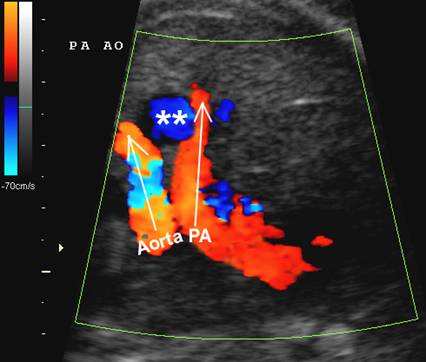
- Enlarged dilated vascular structure between the bifurcation of the main pulmonary artery and descending aorta (4).
- The descending aorta may be dilated.
- The main pulmonary arteries, aorta and neck vessels are normal.
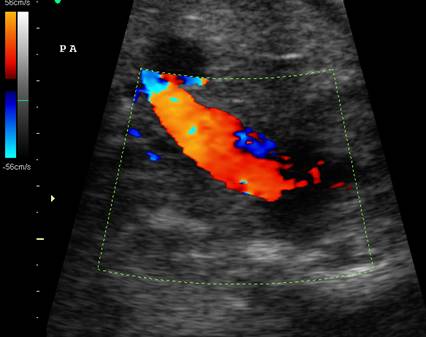
- Color doppler demonstrates turbulent flow from the pulmonary artery to the descending aorta (4).
- Spontaneous resolution has been described postnatally (4).
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|




DIFFERENTIAL DIAGNOSIS |
- Pulmonary artery aneurysm with absent pulmonary valve syndrome.
- Tortuous, non-aneurysmal ductus arteriosus (associated with low blood flow from the pulmonary artery to the aorta in pulmonary atresia, transposition of the great vessels, severe pulmonary stenosis and VSD)(6).
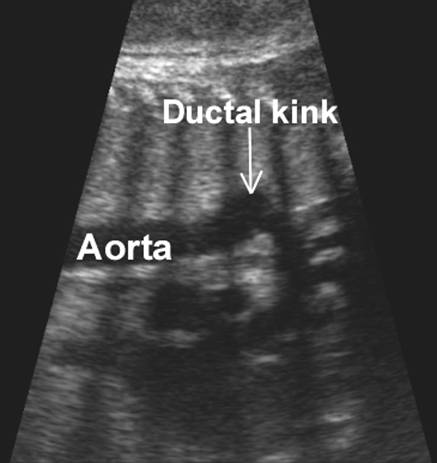
- Exaggerated ductal kink.
|
|
|

|
COMPLICATIONS |
Neonatal complications (1) include:
- Rupture (9%).
- Erosion into bronchus or esophagus (2%).
- Thromboembolism (12%).
REFERENCES |
- Lund JT,
- Laurin S, Sandstrom S, Ivancev K et.al. Ductus arteriosus aneurysm imaging using modern diagnostic methods. Acta Radiol 1992;33:285-291.
- Malone PS, Cooper SG, Elliott M et.al. Aneurysms of the ductus arteriosus. Arch Dis CHILD 1989;64:1386-1388.
- Puder
KS, Sherer DM,
- Crisfield RJ. Spontaneous aneurysm of the ductus arteriosus in a patient with Marfan's syndrome. J Thorac Cardiovasc Surg 1971;62:243-247.
- Hiraishi S, Horiguchi Y, Fujino N et.al. Two-dimensional and doppler echocardiographic assessment of variable shaped ductus arteriosus by the parasternal approach. Pediatr Cardiol 1991;12:6-12.