|
CARDIAC RHABDOMYOMAS |
Cardiac rhabdomyomas are benign smooth muscle hamartomas (1-15), and vary in size from millimeters to several centimeters.
- A single cardiac rhabdomyoma is associated with tuberous sclerosis in 30-50% of cases (1,2). In cases of multiple cardiac rhabdomyomas, approximately 70% have tuberous sclerosis (2).
- 50-60% of patients with tuberous sclerosis have cardiac rhabdomyomata (1,3).
- Rhabdomyomas are the most frequent intracardiac mass (58%), with a reported prevalence of up to 0.25% in autopsy series and 0.08% in live-born infants (14,15).
PATHOPHYSIOLOGY |
ULTRASOUND |
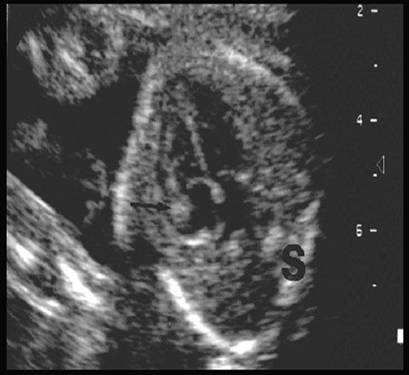
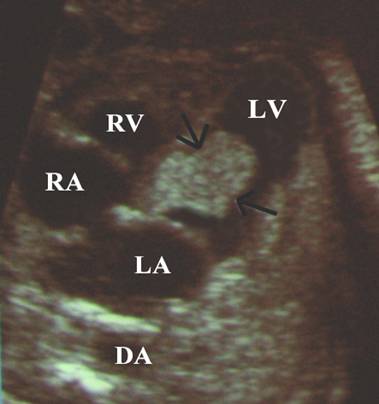
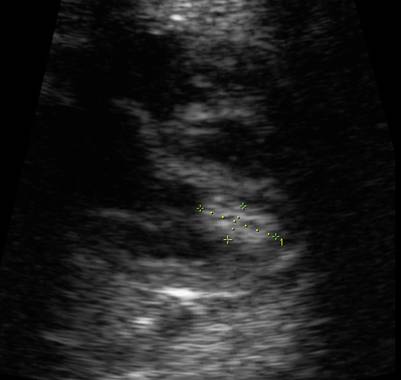
- Solid echogenic masses.
|
Rhabdomyoma in the Right Atrium |
Rhabdomyoma in the Left ventricle |
|
|
|
|
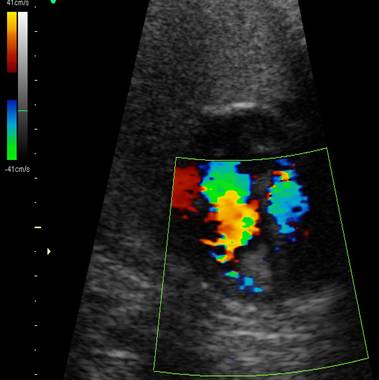
Rhabdomyoma in the right ventricle |
|
|
|
|
|
|
|


- Single or multiple tumors (90%) within the heart (usually arising from the interventricular septum) (1-5). 50% are intracavitary.
- May present as diffuse myocardial thickening (simulating endocardial fibroelastosis (6).
- It occurs with equal incidence in the left and right ventricle and in 30% of cases one or both atria were involved.
- May cause obstruction to the outflow tract or atrioventricular valves, resulting in congestive heart failure, hydrops, pericardial effusion, arrhythmias (7), and supraventricular tachycardia (8,12).
|
|
Video clip of a Rhabdomyoma of the
right ventricle
|

PROGNOSIS |
- The tumour(s) appear to exhibit a biphasic growth. They grow until about 32 weeks of gestation and then shrinks progressively during the first year of life. The period of rapid intrauterine growth has been associated with high gestational hormone concentrations, which might cause hyperplastic and hypertrophic response in the tumors.
- Spontaneous regression has been reported both in utero (9) and childhood (3).
- Sudden death is not uncommon. 60-75% of infants die before reaching their second year (10).
- Prognosis ultimately depends on a variety factors including size, associated arrhythmias, and the exact location of the tumor. Inflow or outflow obstruction (16) may lead to congestive cardiac failure, atrioventricular valve dysfunction with valvular incompetence (11,12)
ASSOCIATIONS |
There is a frequent association with tuberous sclerosis (autosomal dominant).
Prenatal diagnosis of tuberous sclerosis can only be suspected as neonates do
not usually manifest any extracardiac signs until the first year of life. The
only other cardiovascular anomaly associated with tuberous sclerosis is the
rare occurrence of an aortic aneurysm (13).
REFERENCES |
- Bender B, Yunis E. The pathology of tuberous sclerosis. Pathol Annu 1982;17:339-341.
- Smythe JF, Dick JD, Smallhorn JF et.al. Natural history of cardiac rhabdomyomata in infancy and childhood. Am J Cardiol 1990;66:1247-1249.
- Journel H, Roussey M, Plais MH et.al. Prenatal diagnosis of familial tuberous sclerosis following detection of cardiac rhabdomyoma by ultrasound. Prenat Diagn 1986;6:283-289.
- DeVore GR, Hakim S, Kleinman CS et.al. The in utero diagnosis of an interventricular septal cardiac rhabdomyoma by means of real time-directed, M-mode echocardiography. Am J Obstet Gynecol 1982;143:967-969.
- Coates TL, McGahan JP. Fetal cardiac rhabdomyomas presenting as diffuse myocardial thickening. J Ultrasound Med 1994;13:813-816.
- Riggs T, Sholl JS, Ilbawi M et.al. In utero diagnosis of pericardial tumor with successful surgical repair. Pediatr Cardiol 1984;5:23-26.
- Duncan WJ,
- Cha'ban FK, Cohen-Overbeek TE, Frohn-Mulder IM et.al. Multiple intracardiac tumors: spontaneous prenatal recovery of fetal bradyarrhythmia. Ultrasound Obstet Gynecol 1996;8:120-122.
- Spooner E, Ferrina M. Case report: left ventricular rhabdomyoma causing subaortic stenosis: the two dimensional echocardiographic appearance. Pediatr Cardiol 1982;2:67-70.
- Grooves MM, Fagg NLK, Cook
AC et.al. Cardiac tumors in intrauterine life. Arch Dis Child
1992;67:1189-1192.
- Schaffer
RM, Chabbad M, Minkoff H et.al. Sonographic diagnosis of fetal cardiac
rhabdomyoma. J Ultrasound Med 1986;5:531.
- Dennis
MA, Appareti K, Manco-Johnson ML et.al. The echocardiographic diagnosis of
multiple fetal cardiac tumors. J Ultrasound Med 1985;4:327-329.
- McAllister
HA. Primary tumors of the heart and pericardium. Pathol Annu
1979;14:325-355.
- Axt-Fliedner R, Qush H, Hendrik H-J et.al. Prenatal diagnosis of cerebral lesions and multiple Intracardiac rhabdomyomas in a fetus with tuberous sclerosis. J Ultrasound Med 2001;20:63-67.