|
AORTIC STENOSIS |
CLASSIFICATION |
- Supravalvular (occurs above the sinus of Valsalva).
- Associated with William's syndrome.
- Valvular - 60-75%.
- Associated with unicuspid or bicuspid aortic valve and chromosomal abnormalities. Fetuses often develop hydrops in utero.
- Males are affected three to four times more commonly than females.
Critical aortic stenosis |
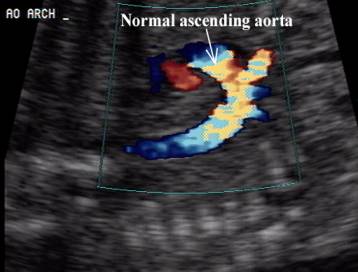
Normal aorta
|
|
|
|
|
|
|
|
|
|
|
|
|
|






- Subvalvular - 8-20%.
- Associated with inherited disorders, asymmetric septal hypertrophy, hypertrophic obstructive cardiomyopathy.
- Males are affected two to three times more commonly than females.
- Dynamic form has been diagnosed in utero.
- Transient form in infants of diabetic mothers.
- 50-60% have associated cardiac lesions.
ULTRASOUND |
- Supravalvular type has not been reported in utero.
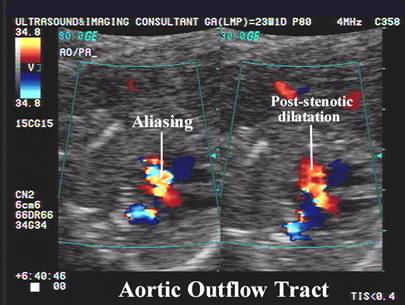
- Thickened aortic valve and doming of the aortic cusps in valvular type.
- Post-stenotic dilatation of the aorta.
|
|
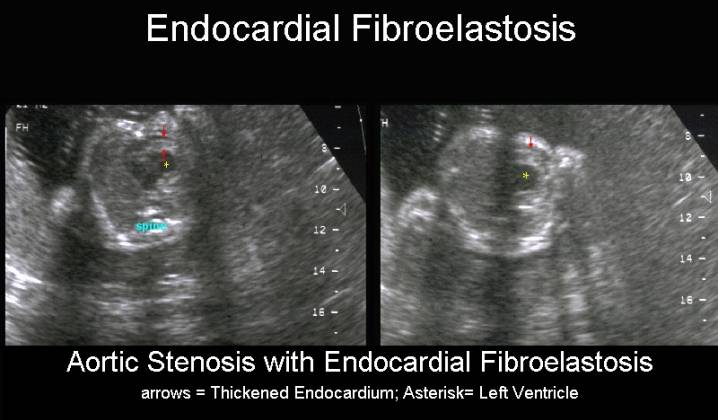
- Thickening of the interventricular septum may be seen in subvalvular aortic stenosis. Asymmetric septal hypertrophy has been identified antenatally (1).
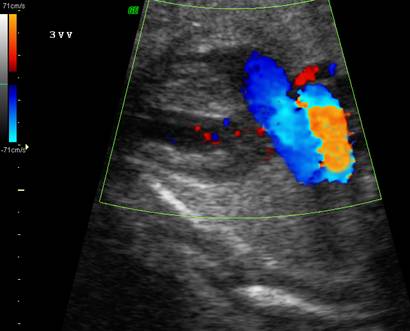
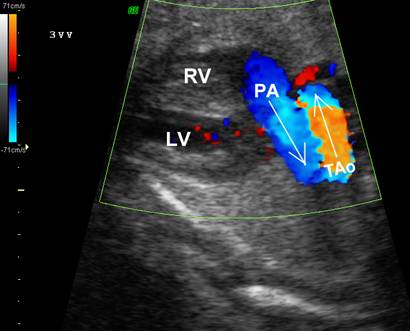
- Doppler may demonstrate post-stenotic turbulence. Peak velocities in the ascending aorta as well as incompetence of the atrioventricular valves may be demonstrated. One can determine the peak velocity as well as the pressure gradient and thus the severity of the stenosis. Flow velocities are usually 1.0-1.2 m/sec across the stenotic valve.
- Although the subvalvular and subaortic types are not usually manifested in the neonatal period, the valvular type may cause cardiac failure in the fetus (2).
- Aortic stenosis is the most common congenital cardiac defect that is found in association with IUGR (3).
- Coarctation of the aorta and interrupted arch are more commonly present making assessment of the entire arch mandatory.
|
|
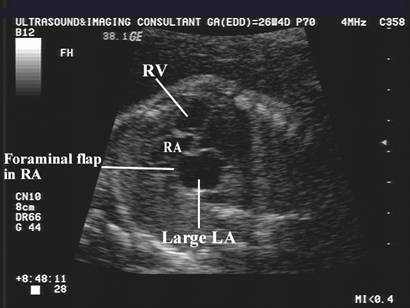
Critical Aortic Stenosis ·
Large LA. ·
Echogenic ·
Compressed RA. |
|
Aortic
stenosis: ·
Large LA on four-chamber view. ·
Foraminal flap moves
from LA to RA (abnormal). ·
Aliasing in the ascending aorta on color doppler. ·
Some post-stenotic dilatation. ·
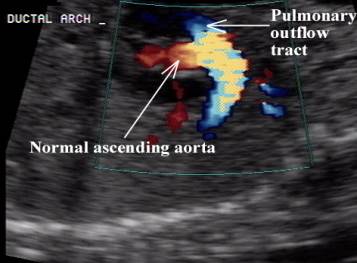
Normal aortic arch and ductal
arch views. ·
Infant died on day 2 from critical aortic stenosis prior
to surgical correction. |
|
|
|
|
|
|
|
|
Retrograde flow in the transverse aortic
arch via the ductus arteriosus |
|
|
|
|



REFERENCES |
- Stewart PA, Buis-Liem T, Verwey RA et.al. Prenatal ultrasonic diagnosis of familial asymmetric septal hypertrophy. Prenat Diagn 1986;6:249-256.
- Allan LD, Little D, Campbell S et.al. Fetal ascites associated with congenital heart disease. Case Report. Br J Obstet Gynecol 1981;88:453-455.
- Reynolds JL. Intrauterine growth retardation in children with congenital heart disease. It's relation to aortic stenosis. Birth Defects Original Article Series 1972;8:143-157.
- Andrisy LS. Prenatal diagnosis of critical aortic stenosis. JDMS 1994;10:332-336.