|
ULTRASOUND OF CHOROID
PLEXUS CYST |
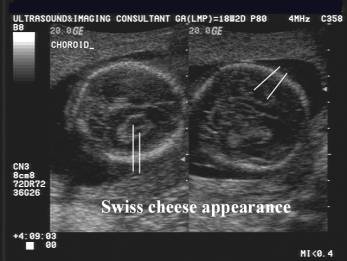
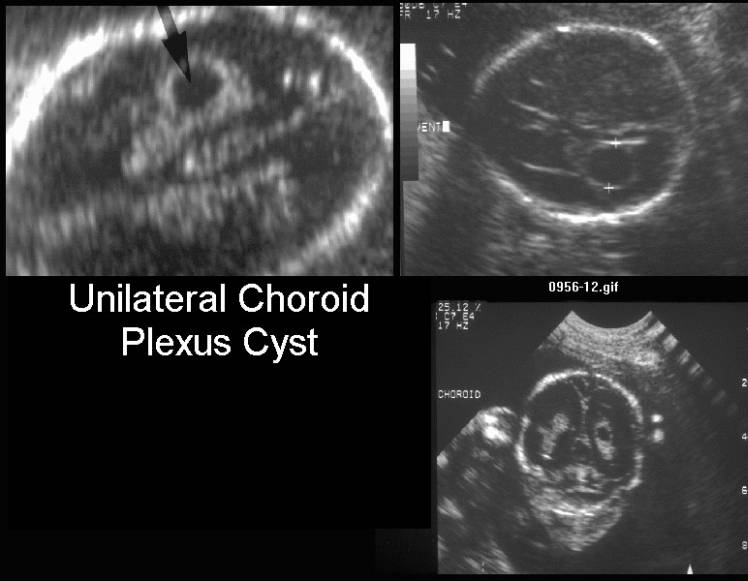
- Sonolucent structure within the highly echogenic choroid plexus. Differentiate the “Swiss cheese” appearance from true choroid plexus cysts.
|
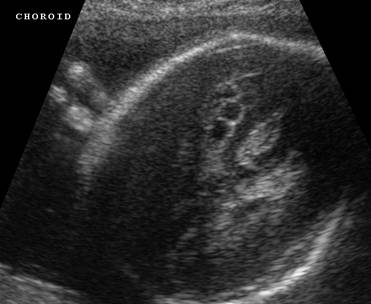
Normal development of the choroid
plexus. The small ill-defined hypoechogenic
cystic areas within the choroid are not true choroid plexus cysts. The “swiss-cheese”
appearance is due to trapped fluid (csf) in the
developing choroid. |
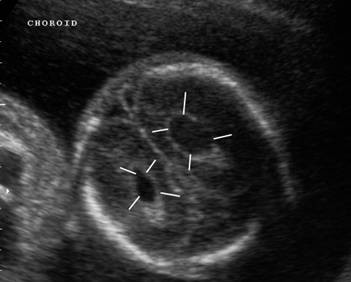
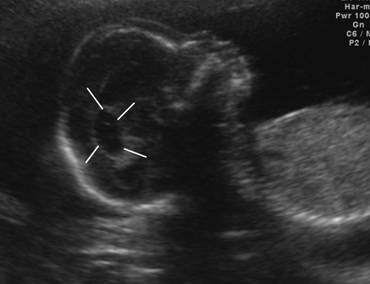
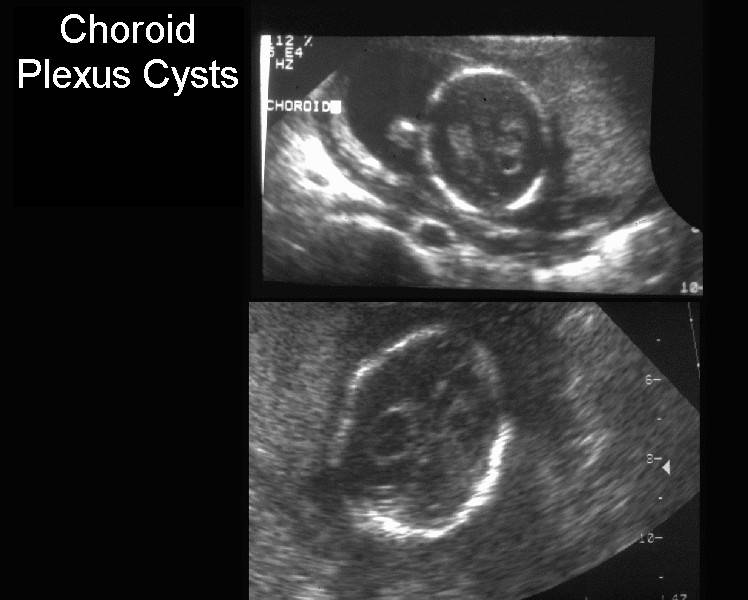
True
choroid plexus cysts
Anechoic,
well-defined, echodense periphery. |
|
|
|
|
|
|



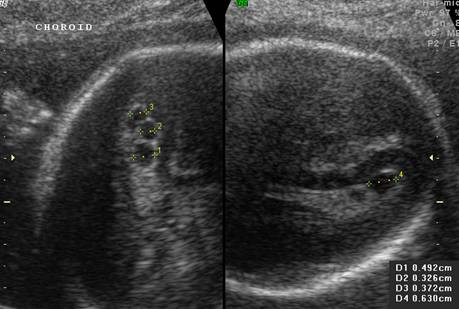
- 3mm or above.
- Variable size
(3mm-20mm).
|
9.1 mm |
14.7 mm |
|
|
|
|
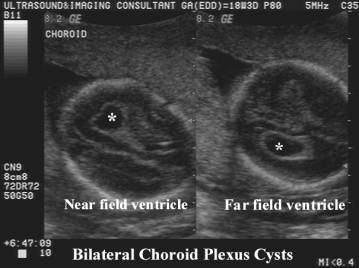
Large
bilateral choroids cysts |
|
|
|
|


- Unilateral / bilateral
Unilateral CPC
|
Bilateral CPC |
|
|
|
|
|
|
|
|
|

- Single cyst / Multiple choroid plexus cysts / Multilocular
cyst.
Multilocular CPC’s
|
|
|
|
|
|
Multiple
CPC’s |
|
|
|
|
|
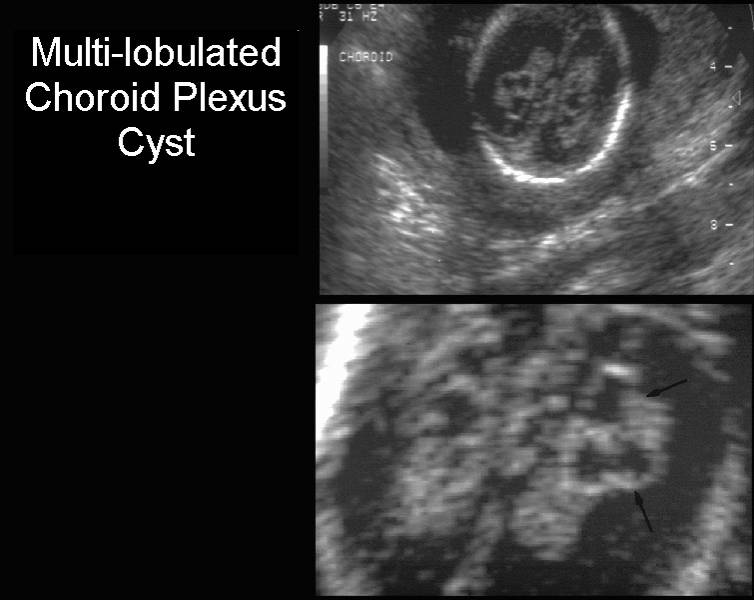
Multilobulated CPC’s |
|
|
|
|


- May contain debris or other small cyst like structures and septations
- Isolated or associated with other structural abnormalities.
- Trisomy 18
- Trisomy 21 (controversial).
- Cri du chat 5p-.
- Mosaic Trisomy 9.
ULTRASOUND ASSESSMENT |
- Isolated
cyst / Cyst associated with other structural anomalies
- Size
of cyst
- Single
versus multiple cysts
- Internal
structure of cysts
- Timing
of cyst resolution
- Detailed scan for other markers (esp of trisomy 18), including fetal echocardiogram.
- Any additional markers …. Genetic counseling and amniocentesis.
- Patient > 35 years … amnio (because of the age-related risk of aneuploidy).
- If the CPC seems to be isolated, and the patient is under the age of 35, the patient's risk of having an affected fetus should be modified with all the available information, specifically maternal age, the presence or absence of other sonographic abnormalities, and the results of the multiple marker screen.
- The estimates calculated by Gratton et al are used to quantify more precisely an individual patient's risk and amniocentesis is recommended when the modified risk exceeds the procedure-related loss rate of amniocentesis (1).
- It is not the presence of a CPC that puts the fetus at risk, but its association with aneuploidy. In the karyotypically normal fetus, the presence of isolated second-trimester CPCs is not associated with any long-term effects, such as mental retardation, cerebral palsy, or delayed development (2).
- Follow-up ultrasounds are not generally needed, because most CPCs resolve. A follow-up ultrasound for growth may be considered in the high-risk patient who declines invasive testing, because trisomy 18 is often associated with IUGR. For a karyotypically normal fetus, CPCs are not associated with adverse pregnancy outcomes; ultrasounds for growth and antenatal testing are not necessary.
REFERENCES |
1.
Gratton RJ,
2. Digiovanni LM, Quinlan MP, Verp MS. Choroid plexus cysts: infant and early childhood developmental outcome. Obstet Gynecol 1997;90:191-4