|
PROXIMAL FOCAL
FEMORAL DEFICIENCY |
Proximal femoral focal deficiency, PFFD, is a congenital anomaly of the
pelvis and proximal femur which causes hip deformity and shortening and altered
function of the involved lower extremity. The condition may be unilateral or
bilateral and is often associated with other congenital anomalies
EMBRYOLOGY |
The developing human embryo first shows evidence of limb buds at the 5
millimeter crown-rump stage.As the apical mesoderm proliferates the limb is
laid down in a proximo-distal fashion to be complete at the 12 millimeter
stage. Elements of the ileum and proximal femur develop from a common
cartilaginous anlage, with subsequent cleft formation to create a joint cavity.
This means that if an acetabulum is seen in radiograph at any time in the first
year of life a femoral head and neck will be present also, even if not evident
in the radiograph
ETIOLOGY |
Numerous agents including irradiation, anoxia, ischemia,
mechanical or thermal injury, bacterial toxins, viral infection, chemicals and
hormones have been postulated as a cause. However, only the drug thalidomide
has been showed to be a definitive cause. When it was taken 4 to 6 weeks after
conception, during the period of limb bud formation and differentiation, major
limb deformities were produced.
CLASSIFICATION |
Gillespie & Torode
classification:
Group (I): ( congenital short femur )
- The involved leg is
not as short as in true PFFD; the foot is at approximately mid tibial level
in relation to the uninvolved limb.
- The leg is flexed,
abducted, and laterally rotated.
- Anteroposterior laxity
of the knee with valgus deformity.
- X ray: the femoral
head and neck are in varus and in retroversion.
- In this group the knee
and the hip can be made functional and, in some patients at least, leg
equalization is possible.
Group (II): ( true PFFD)
- A tenuous
cartilaginous bridge exists between the proximal shaft and the femoral
head.
- The thigh is extremely
short ( overall discrepancy is 35%-50% )
- The leg is held in
abduction and external rotation.
- Flexion contracture of
both hip and knee.
- Surgical procedures
are design to facilitate the fitting of the prosthesis.
|
Aitken classified PFFD
into 4 types on the basis of radiographic features: |
|||
|
Type (A) |
|||
|
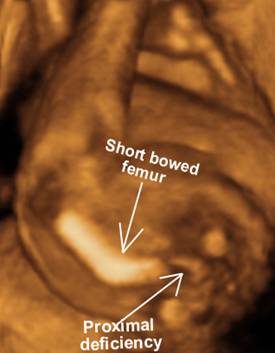
The
femur is short with coxa vara and lateral bowing of its upper third. There
is always adequate acetabulum that contains the femoral head. At
the Subtrochanteric region a pseudoarthrosis develops. At
the skeletal maturity, ossification of the pseudoarthrosis will take place in
most cases, but the varus angulation may be
very severe. Normal acetabulum with located femoral head,
subtrochanteric femoral varus with pseudoarthrosis which usually ossifies by skeletal maturity |
|||
|
|
|
||
|
|
|||
|
Type B |
|||
|
The
ossification of the capital femoral epiphysis is delayed and the acetabulum
is mildly dysplastic. The upper
end of the femoral shaft lies above the femoral head. The
junction between the femoral head and shaft is by defective cartilage that
fail to ossify at skeletal maturity. Normal acetabulum and located femoral head. No osseous connection
between the femoral head and shaft. The femoral shaft usually lies superior to the acetabulum and has a tufted proximal end. |
|||
|
|
|||
|
|
|||
|
|
|
||
|
Type (C) |
|||
|
The
acetabulum is markedly dysplastic and the femoral head never ossify. The femoral
shaft is very short and its upper end tapers sharply to a point. The
hip is very unstable. Dysplastic, flat acetabulum, absent femoral head, short femoral shaft
with proximal tuft with no articulation between the femur and acetabulum. Dysplastic acetabulum Absent
fibula |
|||
|
|
|
||
|
|
|
||
|
|
|
||
|
Type (D ) |
|||
|
Both
acetabulum and femoral head are absent. The
femur is represented by the femoral condyles. Dysplastic, flat acetabulum, absent femoral head, very
short or absent femoral shaft with articulation between the femur and acetabulum |
|||
|
|
|
||
|
|
|
||
|
|
|
||
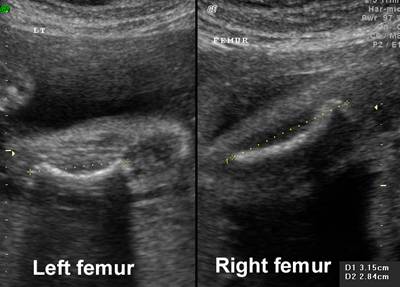
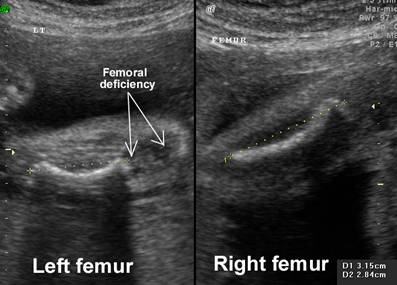


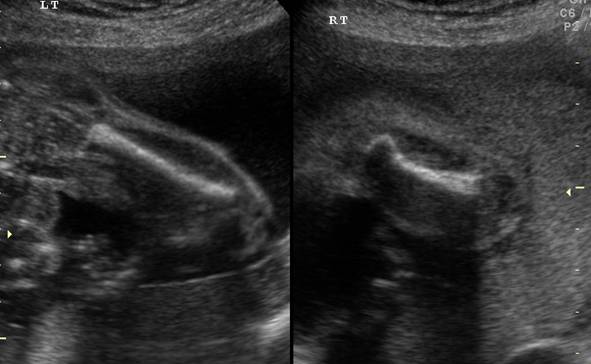








ULTRASOUND |
- One or both femurs may be affected.
- Right femur more commonly involved than the left.
- Anomalies of the upper limb may also be present
ASSOCIATED ANOMALIES |
- Congenital fibular
hemimelia ( 50%-80& )
- Shortening of the
tibia and fibula.
- The patella may be absent
or small and high riding.
- The patellofemoral
joint may be laterally subluxated or dislocated.
- Flexion deformity of
the knee genu valgum.
- Unstable knee joint.
- Foot malformation;
mild hypoplasia, absence of rays, tarsal coalition, talipes equino varus,
or vertical talus.
- Contralateral lower
limb and upper limb deformities.
DIFFERENTIAL DIAGNOSIS |
If both femurs are affected, it is important to carefully examine the face
and exclude femoral hypoplasia-unusual facies syndrome.
REFERENCES |
- Hamanishi C. Congenital short femur. J Bone Joint Sur (Am) 1980;62:307.
- Graham M. Congenital short femur. Prenatal sonographic diagnosis. J Ultrasound Med 1985;4:361.