|
ULTRASOUND OF
ACHONDROPLASIA |
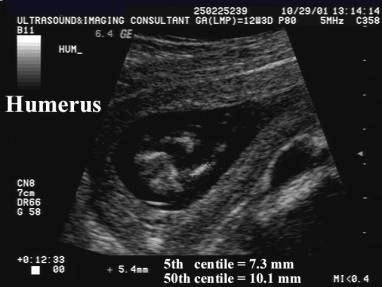
The specific prenatal diagnosis of achondroplasia can be challenging (1). Doray et al (2) correlated prenatal ultrasound (US) with postnatal diagnoses in 47 fetuses with skeletal dysplasia and found it difficult to accurately diagnose the specific skeletal dysplasia. However, in 96% of the cases, they were able to separate lethal from nonlethal skeletal dysplasias. Lethal skeletal dysplasias such as type II osteogenesis imperfecta and thanatophoric dysplasia present early with long bone measurements falling far below the fifth percentile for gestational age by the second trimester. With achondroplasia, limb measurements are typically normal in the first and early second trimester. Drop off of femoral and humeral measurements may be noted at 20 to 24 weeks with a more marked decrease in growth rate apparent in the third trimester (1).
The key to distinguishing between homozygous and heterozygous achondroplasia is careful observation of growth in the second trimester (it is this trimester that the fetus demonstrates much less interval growth of the femur than expected) (3).
- At 26 weeks BPD age:
- Homozygous fetuses never had a femoral length that exceeded 34 mm. (progressive decrease in relative femoral length in the second trimester)
- Heterozygous fetuses always had a femoral length that exceeded 34 mm.
- Fetal femoral growth curves therefore allows the distinction between homozygous, heterozygous and unaffected fetus in the second trimester (1).
Ultrasound |
|
|
·
First Trimester Findings
|
|
|
·
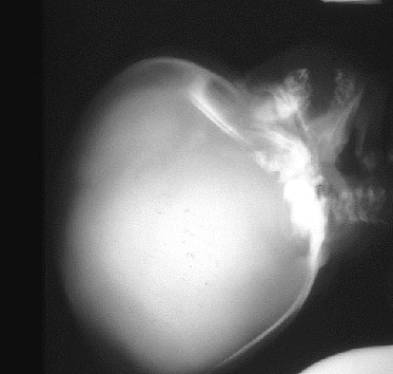
Skull: o
Depressed nasal
bridge. o
Large skull with a
short base. (small foramen magnum which ultimately
results in communicating hydrocephalus due to obstruction of the basal cisterna and aqueduct). o
Relative prognathism. o
Broad mandible. o
Hypoplasia of midface (maxilla). o
Dental malocclusion.
|
|
|
·
Extremities: ·
Rhizometric micromelia o
shortened limbs o
proximal > distal
shortening o
Normal bone
mineralization. o
No bone fractures. o
Predominantly rhizomelic shortening of long bones (femora and humeri). o
Limb bowing. o
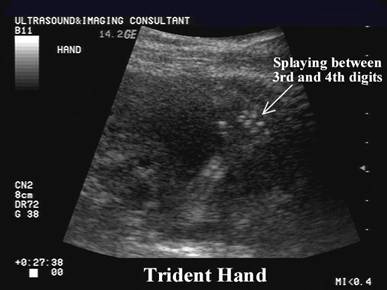
Trident hand. (separation of 2nd
and 3rd digit and inability to approximate 3rd and 4th
finger). o
Brachydactyly (uniform length of short bones of hand) + trident hand.
·
Elbows - lack of
full extension and supination ·
Legs - genu varum (bowleg)
|
|
|
Increased BPD, HC, HC:AC ratio. |
|
|
Normal thorax and
cardio-thoracic ratio. |
|
|
·
Homozygous form: o
Short ribs with
flared ends. o
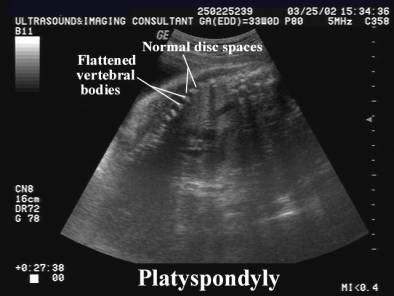
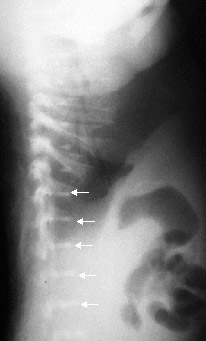
Hypoplastic vertebral bodies (platyspondyly). o
Flat acetabular roof and small sciatic notches.
·
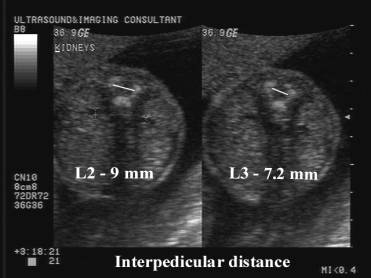
Interpedicular distance decreases from L1 to L5.
|
|
|
Spine: ·
Thoracolumbar - kyphotic ·
Lumbar - lordotic |
Pelvis:
|












REFERENCES |
- P. Modaff,
V.K. Horton and R.M. Pauli, Errors in the
prenatal diagnosis of children with achondroplasia.
Prenatal Diagnosis 16
(1996), pp. 525–530.
- B.
Doray, R. Favre, B. Viville et al., Prenatal sonographic
diagnosis of skeletal dysplasias. Ann Genet 43 (2000), pp. 163–169.
- Patel
MD, Filly RA. Homozygous achondroplasia: