|
ANOMALIES OF THE ANTERIOR NUCHAL REGION |
- Most normal structures of the anterior neck, especially the thyroid gland, carotid sheath, upper airway and trachea are small and barely visible. Abnormalities arising anteriorly therefore usually evident although rarely encountered.
- Fetal neck is usually held in a neutral position; marked hyperextention (in the absence of iniencephaly or torticollis) warrants a careful search for an anterior or laterally situated mass.
- Detection of anteriorly situated lesions are important as even small lesions can compress the airways necessitating urgent post natal intubation.
- Antenatal differentiation, although not always possible, is based on:
- Position of the lesion.
- Sonographic characteristics: solid, cystic, mixed, calcified or vascular.
- Relationship to the major vessels of the neck.
- Associated abnormalities - polyhydramnios, fetal tumor elsewhere eg adrenal gland, or bony abnormalities.
CENTRAL MIDLINE ANTERIOR NUCHAL LESIONS
S – SOLID; C – CYSTIC; M - MIXED |
Lesion
|
Ultrasound Appearance |
Relationship to jugular v. and carotid artery |
Other comments
|
|
|
S/C/M |
Other features |
|||
|
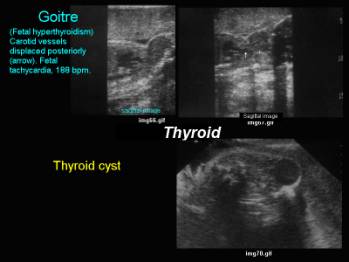
Goiter |
S |
Fetal tachycardia IUGR, advanced bone age. |
Anteromedial |
Associated with maternal
thyrotoxicosis or congenital cretinism. |
|
|
|
|
||
|
Thyroid Cyst |
C |
|
Anterior |
Associated with maternal
thyrotoxicosis. May arise laterally and be confused with a branchial cleft cyst. |
|
|
|
|
||
|
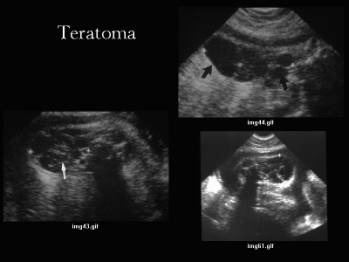
Teratoma |
S C M |
± calcium. Marked neck hyperextention Polyhydramnios (30%) |
Anteromedial |
Enlarges rapidly. Vascular
but no venous lakes helps distinguish from
hemangioma. 80% die without post- natal resection. |
|
|
|
|
||
|
Thyroglossal duct cyst (34-37) |
C |
Located below mandible but is otherwise similar to lymphangioma |
Anterior or anteromedial |
75% midline |
|
|
|
|
||
|
Laryngocele |
C |
|
Medial |
Indistinguishable from thyroglossal duct cyst |
|
|
|
|
|
|
|
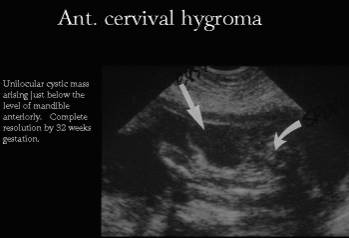
Hygroma |
C |
Usually non septated No hydrops |
Anterior |
Usually isolated Resolves
spontaneously No relationship to Aneuploidy or XO. |
|
|
|
|
|
|
|
S C |
Polyhydramnios Echogenic lungs |
Medial |
Trachea usually visualized, as it is fluid filled. |
|
|
Hemangioma (33,34) |
S C M |
Color flow on pulsed
doppler |
Usually anterior |
MRI helful in planning
treatment |
|
Lingual lymphangioma (35,36) |
C M |
Appearance dependent on
ehich subtype predominates (capillary;cavernous;cystic hygroma). |
Anaterior |
Thin walled multiseptated
hypoechogenic mass. Size varies from small
collections of fluid to large cysts. |
|
Cervical meningocele /
anterior encephalocele (34-36) |
C |
Spinal defect may be
difficult to demonstrate antenatally. |
|
|
|
Congenital epulis (38-39) |
S |
Single or multiple Found on maxillary alveolar
ridge or mandible |
|
Congenital gingival
granular cell tumor Benign intraoral tumor Cases have only been
detected in late second or third trimester. |
|
Congenital ranula (38-40) |
C |
Indistinuishapble fro other
cystic lesion by Sonography alone |
|
Dilatation of the
sublingual and submandibular ducts in the floor of the mouth. Classified according to
location:
|
|
Intra-oral duplication
cysts (41-43) |
C |
Tend to occur in the floor
of the mouth. |
|
1.8% of alimentary tract
duplications were noted in the cervical region in one study. May not be diagnosed for
years if they are small and symptomatic. |


|
FETAL GOITER (9-15) |
Antenatal diagnosis is essential as timely recognition and treatment is essential to achieve normal growth and neurological development. Untreated fetal hypothyroidism may result in mental retardation, language, motor and spatial problems, growth retardation, congenital heart block and delayed skeletal maturation.
A large fetal thyroid gland may also result in fetal malposition due to hyperextension of the neck, tracheal obstruction, esophageal compression and polyhydramnios, neonatal asphyxia and death.
Risk factors for fetal goiter (goiter in the fetus may be due to either hypothyroidism or hyperthyroidism):
1. Previous medical therapy for hyperthyroidism.
2. Previous high dose irradiation of the neck.
3. Thyroid autoimmune disease (thyroiditis).
4. Family history of thyroid disease.
5. Treatment with amiodarone.
6. Type I maternal diabetes mellitus.
7. Hypopituitarism.
Fetal Hypothyroidism:
Transient fetal hypothyroidism is most frequently associated with maternal ingestion of anti-thyroid drugs (propylthiouracil –PTU; carbimazol; I-131 in pregnant women).
Fetal Hyperthyroidism is usually secondary to maternal autoimmune disease. In Graves disease the mother produces several IgG thyroid stimulating immunoglobulins which can cross the placenta and cause fetal hyperthyroidism.
|
CERVICAL TERATOMA |
Fetal teratomas consist of ectodermal, endodermal and mesodermal germ-cell tissue including central nervous tissue. Mature and immature teratomas are distinguished by the degree of differentiation of the tissue.
Cervical teratomas in the fetus are rare. They have an incidence of 1 in 20 000–40 000 live births and account for about 6% of all fetal teratomas (16-18). Airway obstruction in the newborn because of tracheal compression or occlusion has been reported as the cause of an 80–100% mortality rate in untreated cervical teratomas in the neonatal period(19-21). Other researchers in the last decade have reported mortality rates of approximately 20–30% (22-24).
Usually fetal cervical teratomas are considered benign; however, the malignant transformation of fetal cervical teratomas has been reported (20).
ULTRASOUND
|
- The sonographic findings of cervical teratomas typically include solid and cystic structures within a heterogeneous mass mass.
- In up to 50% of cases calcifications might be seen within the mass while cartilage or bone tissue is less common (25).
- Polyhydramnios due to impairment of fetal swallowing might be seen in up to one third of the cases.
- The extent of vascularization can be assessed by Doppler flow imaging.
- Magnetic resonance imaging has also been described as providing essential information about the diagnosis and the anatomy of giant fetal neck masses and the adjacent airway (26).
ASSOCIATED MALFORMATONS
|
Associated malformations are rare, although there have been reports of lung and upper airway hypoplasia (19, 23).
DIFFERENTIAL DIAGNOSIS
|
- cystic hygroma,
- lymphangioma,
- hemangioma
- cervical meningocele
- thyroglossal duct cyst
- esophageal diverticula
- dermoid cyst
- brachial cleft cyst
- epignathus
- congenital goiter.
OUTCOME
|
Jordan and Gauderer reviewed 194 cases of fetal teratoma without regard to the prenatal diagnosis (20). They reported an overall mortality of 37% with 15% of the cases being stillborn or moribund at delivery. Fifty-one percent of the fetuses were born with severe respiratory distress and 43% of those fetuses subsequently died. Furthermore, in 13% of cases that underwent surgery, the newborns died from surgical complications or metastasis. In 2% of the 194 cases the teratoma was malignant.
According to more recent literature the reported mortality and morbidity of cases with fetal teratoma has decreased (22): the mortality rate has decreased to 18% and in only 33% of cases was severe respiratory distress present at delivery. Mortality due to operative treatment has reduced to 4%. Whether improved prenatal and perinatal management or bias due to selection of reported cases accounts for these data has to be established.
Axt-Fliedner and Hendrik (27) report the unfavorable outcome of a fetus with a giant teratoma which extended to the anterolateral right aspect of the neck and thorax. After Cesarean section a patent fetal airway could not be established.
|
LARYNGEAL CYSTS (48-54) |
Laryngeal
cysts in
children:
- Aryepiglottic cysts
represent the most common
- Vallecular cysts or
pre-epiglottic cysts are lesscommon
Vallecular
cysts (mucous
retention cyst, epiglottic cyst, base-of-the-tongue cyst and more recently
ductal cyst.
- Benign, but may cause
airway obstruction and even death if not treated appropriately (a
mortality rate of about 40% in children has been reported.
- They are unilocular, of
variable size arising from the lingual surface of the epiglottis and
containing clear, non-infected fluid.
- Probably result from
obstruction of mucous glands at the base of the tongue.
- They are lined with
mucous glands and therefore as mucous secretion continues the lesion
gradually increases in size.
- Vallecular cysts with
respiratory epithelium are rare.
- Embryology:
o
The
respiratory system appears as an endodermal outgrowth from the ventral wall of
the foregut immediately caudal to the hypobranchial eminence (when the embryo
is approximately 3 weeks old).
o
The
ventrally placed respiratory bud then becomes separated from the dorsal
portion, the esophagus, except at the entrance to the larynx, where it
maintains its communication with the foregut through the laryngeal orifice.
o
The
remaining part of the gut contributes to the development of the stomach and
duodenum, just caudal to the liver.
o
Because
of the proximity of the primitive gut and the pharyngeal arches, which contain
the developing tongue, embryonal remnants of the gut may appear in the tongue.
These epithelial remnants may subsequently contribute to the development of
cystic lesions of the tongue.
·
Vallecular
cysts are rarely associated with other fetal anomalies.
·
Complications
include polyhydramnios; pulmonary hypoplasia; trachea, cervical vessels and
hypoglossal nerve compression.
·
Differential
Diagnosis – see table above.
|
CONGENITAL RANULA (29-30) |
- Results from a dilatation of the sublingual or submaxillary gland ducts in the floor of the mouth.
- These pseudocysts are normally located in the sublingual space between the mylohyoid muscle and the lingual mucosa, and can be classified according to their localization:
- simple ranulas (in the floor of the mouth)
- cervical ranulas (in the paracervical area)
- plunging ranulas near the superior airway.
- ultrasonographically they are indistinguishable.
|
MUCOCELES (31) |
- Mucoceles of the oral cavity refer to collections of mucus resulting from obstruction of, or leakage from a major or minor salivary gland.
- Mucoceles occur commonly in the oral cavity, typically on the lower tip but also in unusual locations, such as in young patients.
|
HETEROTOPIC GASTROINTESTINAL CYST (32) |
· Intra-oral duplication cysts of the alimentary tract are rare. They tend to occur in the floor of the mouth or within the tongue.
· 1,8 % of alimentary tract duplications were noted to be in the cervical region. They are usually diagnosed in the newborn period but may be undetected for years if asymptomatic and small.
|
VALLECULAR CYSTS (44-48) |
· Sporadic.
· Most likely result from obstruction of mucous gland at the base of the tongue.
· Lined with mucous glands and with continued mucous secretion, the lesion gradually increases in size.
· Vallecular cyst is considered to be more common in adults than children.
- Because of the proximity of the primitive gut and the pharyngeal arches, which contain the developing tongue, embryonal rests of the gut may become misplaced in the developing tongue. It is believed that these epithelial remnants may subsequently contribute to the development of cystic lesions of the tongue.
REFERENCES
|
- Pearlman AH, Johnson RL, Clemons RD et.al. Intrauterine Diagnosis and Treatment of Fetal Goitrous Hypothyroidism J Clin Endocrinol Metab 1990; 71:618-621
- Weiner S, Scharf JI, Bolognese RJ, Librizzo. Antenatal Diagnosis and Treatment of a Fetal Goiter The Journal of Reproductive Medicine 1980; 24:39-42
- Avni EF, Rodesch F, Vandemerckt C et.al. Detection of a Fetal Goitre by Ultrasound Br J Radiol 1992; 65:302-305
- Vali A, Wiles P, Thomas NB et.al. Relapse of Maternal Thyrotoxicosis presenting as a second trimester goiter Ultrasound Obstet Gynecol 1993;3:429-431
- Bromley B, Frigoletto FD, Cramer D et.al The Fetal Thyroid: normal and abnormal sonographic measurements. J Ultrasound Med 1992; 11:25-28
- Rosenfeld CR, Coln CD, Duenhoelter JH. Fetal Cervical Teratoma as a Cause of Polyhydramnios. Pediatrics 1979; 64:176-178
- Brohnstein M, Bar-Hava I Blumenfeld I et.al. The difference between septated and nonseptated nuchal cystic hygroma in the early second trimester Obstet Gynecol 1993; 81:683-687
- Suchet I Ultrasound of the
Fetal Neck in the second and third trimester. Part 3. Anomalies of the
anterior and anterolateral nuchal region Can Assoc Radiol J 1995;
46:426-433
- Hadi
HA, Strickland D. In utero treatment of fetal goitrous hypothyroidism
caused by maternal Graves disease. Am J Perinataol 1995;12(6):455-458.
- Van
Loon AJ, Derksen JT, Bos AF et.al. In utero diagnosis and treatment of
fetal goitrous hypothyroidism, caused by maternal use of prpoylthiouracil.
Prenat Diagn 1995;15:599-604.
- Bruner
JP, Dellinger EH. Antenatal diagnosis and treatment of fetal
hypothyroidism. Fetal diagn Ther 1997;12:200-204.
- De
Catte L, de Wolf De, Smitz J et.al. Fetal hypothyroidism as a complication
of amiodarone treatment for persistent supraventricular tachycardia.
Prenat Diagn 1994;14:00-04/
- Bromley
B, Frigoletto FD, Cramer D et.al. The fetal thyroid: normal and abnormal
measurements. J Ultrasound Med 1992;11:25-28.
- Fisher
DA. Fetal thyroid function: diagnosis and management of fetal thyroid
disorders. Clin Obstet Gynecol 1997;40:16-31.
- Nicoli U, Venegoni E, Acaia B et.al. Prenatal treatment of fetal hypothyroidism: is there more than one option? Prenat Diagn 1996;16:443-448.
- Grosfeld JL, Ballantine TVN, Lowe D, Baehner RL. Benign and malignant teratomas in children: analysis of 85 patients. Surgery 1976; 80: 297–305
- Tapper D, Lack EE. Teratomas in infancy and childhood. A 54-year experience at the Children’s Hospital Medical Center. Ann Surg 1983; 198: 398–409
- Azizkhan RG, Haase GM, Applebaum H et. al. Diagnosis, management, and outcome of cervicofacial teratomas in neonates: a children’s cancer group study. J Pediatr Surg 1995; 30: 312–316
- Zerella JT, Finberg FJ. Obstruction of the neonatal airway from teratomas. Surg Gynecol 1990; 170: 126–131
- Jordan RB, Gauderer MWL. Cervical teratomas: an analysis. Literature review and proposed classification. J Pediatr Surg 1988; 23: 583–591
- Schulman SR, Jones BR, Slotnick N, Schwartz MZ. Fetal tracheal intubation with intact uteroplacental circulation. Anaesth Analg 1993; 76: 197–199
- Kerner B, Flaum E, Mathews H et.al. Cervical teratoma: Prenatal diagnosis and long-term follow up. Prenat Diagn 1998; 18: 51–59
- O’Callaghan SP, Walker P, Wake C et.al. Perinatal care of a woman with the prenatal diagnosis of a massive fetal neck tumour (cervical teratoma). Br J Obstet Gynaecol 1997; 104: 261–263
- Kelly MF, Berenholz L, Rizzo KA et.al. Approach for oxygenation of the newborn with airway obstruction due to a cervical mass. Ann Otol Rhinol Laryngol 1990; 99: 179–182
- Gundry SR, Wesley JR, Klein MD et.al. Cervical teratomas in the newborn. J Pediatr Surg 1983; 18: 382–386
- Hubbard AM, Crombleholme TM, Adzick NS. Prenatal MRI evaluation of giant neck masses in preparation for the fetal EXIT procedure. Am J Perinatol 1998; 15: 253–257
- Axt-Fliedner R, Hendrik H –J, Erktan K et.al. Course and outcome of a pregnancy with a giant fetal cervical teratoma diagnosed prenatally. Ultrasound Obstet Gynecol 2001;18:543-546.
- Kin Sun Wong, Hsueh Yu Li, Tsun Sheng Huang—Vallecular cyst synchronous with laryngomalacia : Presentation of two cases. Otolaryngol Head Neck Surg 1995; 13: 621-624.
- Kim E.S., Gross T.L.- Prenatal ultrasound detection of a congenital epulis in a triple X female fetus: a case report. Prenat Diagn 1999;19: 774-776.
- Pellicano M., Zullo F., Catizone C et.al. - Prenatal diagnosis of congenital granular cell epulis. Ultrasound Obstet Gynecol 1998;11: 144-146.
- Crean S.J., Connor C.- Congenital mucoceles : report of two cases. Int J Paed Dent 1996;6: 271-275.
- Chen M.K., Gross E., Lobe T.E.- Perinatal management of enteric duplication cysts of the tongue. Am J Perinat 1997;14:161-3
- Shiraishi H., Nakamura M., Ichihashi K., Uchida A., Izumi A. et al- Prenatal MRI in a fetus with a giant neck hemangioma : a case report. Prenat Diagn 2000 ; 20 : 1007-8.
- Paladini D., Morra T., Guida F., Lamberti A., Martinelli P.- Prenatal diagnosis and perinatal management of a lingual lymphangioma. Ultrasound Obstet Gynecol 1998 ; 11 : 141-3.
- Mahboubi S., gheyi V.- MR imaging of airway obstruction in infants and children. Int J Pediatr Otorhinolaryngol 2001 ; 57 : 219-27.
- Giacalone P.L., Boulot P., Deschamps F., Nagy P., Hedon B. et al- Prenatal diagnosis of a multifocal lymphangioma. Prenat Diagn 1993 ; 13 : 1133-7.
- Urao M., Teitelbaum D.H., Miyano T.- Lingual thyroglossal duct cyst : a unique surgical approach. J Pediatr Surg 1996 ; 31 : 1574-6.
- Kim E.S., Gross T.L.- Prenatal ultrasound detection of a congenital epulis in a triple X female fetus: a case report. Prenat Diagn 1999 ; 19 : 774-6.
- Pellicano M., Zullo F., Catizone C., Guida F., Catizone F., Nappi C.- Prenatal diagnosis of congenital granular cell epulis. Ultrasound Obstet gynecol 1998 ; 11 : 144-6.
- Fernandez Moya J.M., Sulzberger S.C., Diaz Recasens J., Ramos C., Sanz R., Perez Tejerizo G.- Antenatal diagnosis and management of a ranual. Ultrasound
- Crean S.J., Connor C. Congenital mucoceles : report of two cases. Int J Paed Dent 1996 ; 6 : 271-5.
- Chen M.K., Gross E., Lobe T.E.- Perinatal management of enteric duplication cysts of the tongue. Am J Perinat 1997 ; 14 : 161-3
- Gray G.G., Voigt E., Breuer F., Rothman L.M.- Imaging quiz case two. Arch otolaryngol Head Neck Surg 1999 ; 125 : 593-5
- Kin Sun Wong, Hsueh Yu Li, Tsun Sheng Huang—Vallecular cyst synchronous with laryngomalacia : Presentation of two cases. Otolaryngol Head Neck Surg 1995 ; 113 : 621-4.
- Ruben R.J., Kucinski S.A., Greenstein N.- Cystic lymphangioma of the vallecula. Can J Otol 1975 ; 4 : 180-4.
- Guttiérrez J.P., Berkowitz R.G., Robertson C.F.- Vallecular cysts in newborns and young infants. Pediatr Pulmonol 1999 ; 27 : 282-5.
- Manor Y., Buchner A., Peleg M., Taicher S.- Lingual cyst with respiratory epithelium: an entity of debatable histogenesis. J Oral Maxillofac Surg 1999 ; 57 : 124-7.
- Naidoo L.C.D. - Medial lingual cyst: Review of the literature and report of a case. J Oral Maxillofac Surg 1997 ; 55 : 172-5.
- Wong KS, Li HY, Huang TS. Vallecular cyst synchronous with
laryngomalacia: presentation of two cases. Otolaryngol Head Neck Surg
1995; 113: 621-624
- Ruben RJ, Kucinski SA, Greenstein N. Cystic lymphangioma of the vallecula. Can J Otol 1975; 4: 180-184
- Guttiérrez JP, Berkowitz RG, Robertson CF. Vallecular cysts in newborns and young infants. Pediatr Pulmonol 1999; 27: 282-285
- Manor Y, Buchner A, Peleg M, Taicher S. Lingual cyst with respiratory epithelium: an entity of debatable histogenesis. J Oral Maxillofac Surg 1999; 57: 124-127
- Naidoo LCD. Medial lingual cyst: review of the literature and report of a case. J Oral Maxillofac Surg 1997; 55: 172-175
- Shear M. Lingual cyst with respiratory epithelium: an entity of debatable histogenesis. J Oral Maxillofac Surg 1999; 57: 128-129