|
EMBRYOLOGY OF THE
LOWER UROGENITAL TRACT |
- The cloaca is an area of dilatation that is the distal end of the hindgut. It is lined by endoderm. Solid cells from the lateral cell masses move caudally to the anterior portion of the cloaca and canalize into the wolffian ducts at 4 to 5 weeks gestation.
- Soon afterward, a second set of tubes develop laterally from coelomic evaginations and become the Mullerian duct system (MDS).
- The cloaca is closed inferiorly by a cloacal membrane made up of a thin endodermal and a thick ectodermal layer (1-5).
- After the wolffian and mullerian ducts develop and insert into the anterior cloaca, the endodermal tissue of the cloaca is divided by a urorectal (urogenital) septum into a dorsal rectum and an anterior urogenital (UG) sinus. The UG sinus is made up of the cranial, allantoic, and phallic portions.
- The cranial (vesical) portion becomes the bladder, which maintains continuity with the allantois. The allantois eventually closes becoming a thick fibrous band, the urachus that extends form bladder apex to the umbilicus. It is known in the adult as the median umbilical ligament of the inner infraumbilical abdominal wall.
- The caudal portions of the mesonephric ducts incorporate into the dorsal portion of the developing bladder. Endodermal epithelium of the UG sinus soon replaces the initial mesonephric duct tissue making up the developing trigone. Mesonephric ducts eventually are resorbed, with the caudal end of each degenerating in the female but becoming the ejaculatory duct in the male.
- Ureters open separately into the bladder superior and lateral to the ejaculatory ducts (1,3,5).
- The
distal urethra arises by the formation of the urethral folds, which fuse
in the midline in a cranial to caudal direction. The Wolffian
duct is incorporated into the urethral wall of the septum, forming
Muller's tubercle. The portion proximal to Muller's tubercle becomes the prostatic urethra, while the remaining distal portion
of the urogenital sinus develops longitudinal ridges
in its lateral walls (urethrovaginal folds). The
cranial remnants of the urethrovaginal folds
remain on place as plicae colliculi,
and migrate laterally by lateral growth and fusion of the bulbous and
cavernous portions of the urethra.
|
|
|
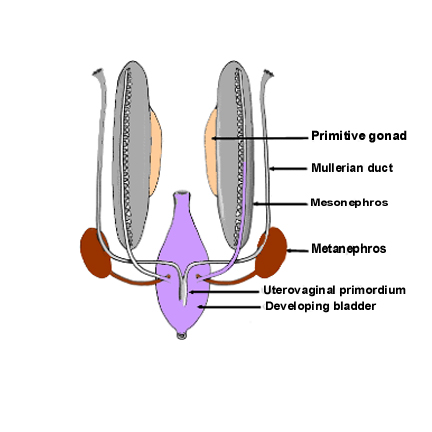
The primitive
gonad differentiates into a testis at 7 weeks of fetal
life only in the presence of the HY antigen found on the Y chromosome.
Without a Y chromosome, differentiation into an ovary begins at 17 weeks
gestation in the presence of 2 X chromosomes |
|
Both sexes
develop 2 different pairs of genital ducts. Parts of the wolffian
or mesonephric duct system develop into the epididymis, vas deferens, and seminal vesicles under the
influence of testosterone. By 6 weeks, a mullerian
(paramesonephric) duct has developed lateral to
each ipsilateral wolffian
(mesonephric) duct |
|
In females, the
MDS develops into the fallopian tubes, uterus, and upper two thirds of the
vagina, and the wolffian system degenerates. If the
MDS is dysgenetic, the uterus or vagina may be
absent or rudimentary as in the Mayer-Rokitansky-Kuster-Hauser
syndrome. By 11 weeks, a Y-shaped uterovaginal primordium has developed into the two fallopian tubes and
with proper MDS fusion a single uterus, cervix, and upper two thirds of the
vagina. This occurs in the presence or absence of ovaries, as long as there
are no testes or high levels of androgens present. The testes produce
testosterone, a masculinizing hormone, and mullerian inhibition factor that suppresses
the further development of the paramesonephric
ducts. |
|
REFERENCES |
- N.R.
Dunnick, C. Sandler,
E.S. Amis, Jr et al.. Textbook of Uroradiology
((ed 2).), Williams & Wilkins,
- K.L.
Moore and T.V.N. Persaud. The Developing Human.
Clinically Oriented Embryology (ed 7.), Saunders,
- R.S. Narlawar, V. Hanchate, A. Raut et al., Renal agenesis and seminal vesicle cyst. J Ultrasound Med 22 (2003), pp. 225–228.
- T.W.
Sadler. Langman’s Medical Embryology (ed 9.), Lippincott Williams
& Wilkins,