|
THE |
ANATOMY |
- Posterior to broad ligament.
- Anterior to iliac vessels and ureter.
- Inferior to uterine tube.
- Held in place by ovarian ligaments and infundibulopelvic (suspensory) ligaments.
- Blood supply:
- Adnexal branch of uterine artery and an ovarian branch, which runs through the infundibulopelvic ligament.
- Almond shaped paired structures on either side of uterus.
- Size of ovaries is related to patients age and phase of follicular development.
- 3-4cm long, 2cm wide and 1cm AP dimension.
- Volume of the ovaries versus age
= 6cm cubed (range = 9.8-10.9cm cubed).
= 3.5cm cubed in postmenopausal patients. - Low-level echo pattern interrupted by anechoic areas that represent developing follicles, functional cysts or corpora lutea.
- Usually found lateral to uterus, but it may be found in other locations due to the flexibility of the round ligament.
- Landmarks:
- Anterior to internal iliac artery.
- Ovarian artery entering superior pole.
- Echo pattern with follicles.
|
Sagittal views of left and right ovary |
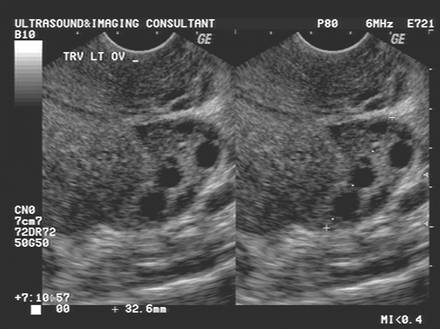
Transverse views of left and right ovaries |
|
|
|
|
|
|
Fimbrae
|
|
|
|
|





OVULATION |
Nakata
et al. (1), studying the corpora lutea in postreproductive but premenopausal
women undergoing hysterectomy, proposed that an ultrasound investigation of the
CL in the mid-luteal phase should use the following
criteria to classify it into one of four types:
- Type A, hypoechogenic
central part with wall of < 3 mm;
- Type B, hyperechogenic
central part with wall of < 3 mm;
- Type C, hypoechogenic
central part with wall of
 3 mm;
3 mm; - Type D, hyperechogenic
central part with wall of 3 mm.
These authors showed a relationship between the ultrasonographic pattern and hormonal milieu, and indeed,
the finding of a hypoechogenic central region with a
thin wall (< 3 mm) may indicate corpus luteal
insufficiency since significantly lower serum progesterone levels were found in
women with this type of CL.
Backstrom,
Nakata and Pierson, in 1994 (2), stated that, the ultrasonographic
evaluation of the CL could add a ![]() tremendous
amount of potentially useful information
tremendous
amount of potentially useful information![]() .
.
Nakata
during the 1992 study, were able to demonstrate that transvaginal
ultrasonography, in combination with intraovarian color Doppler flow measurements, is a simple
and reliable method to evaluate the size and vascularization
of the human CL (3).
Baerwald et
al (4) characterized changes in luteal form and
function using serial transvaginal ultrasonography, gray-scale imaging and analysis of serum
hormonal patterns. The hypothesis that changes in luteal
morphology and endocrine secretion would be detected during the interval
between two subsequent ovulations seems to be supported.
Two
morphological types of CL were observed following ovulation:
·
with a central fluid-filled cavity (CFFC) (78%),
·
without a central fluid-filled cavity (CFFC).
The
incidence of corpora lutea containing a CFFC was
greatest immediately following ovulation and then subsequently declined. Prior
to this study, the physiological significance of the ![]() cystic
cavities
cystic
cavities![]() has not been
well-documented. CFFCs were attributed to the chance
occurrence of follicle rupture across a vascular component of the follicle
resulting in leakage of blood into the follicular lumen. Measurements of the luteal area, defined as the area between the external
border of the CL and the internal border of the CFFC, and luteal
numerical pixel value (NPV) were the main outcome measures of the study. Luteal area seems highly correlated with progesterone
concentrations during the interovulatory interval
(IOI). Luteal area and estradiol
concentrations, however, were not as strongly correlated. The regressing CL was
present in the follicular phase but it did not appear to be functional as
indicated by basal levels of serum progesterone and estradiol.
This study investigated also the quantitative changes
in luteal echotexture that
seems reflective of changes in the morphological and physiological status of the
CL in women. A decrease in luteal NPV occurred during
luteal development in association with an increase in
luteal area, progesterone and estradiol
concentrations, while the subsequent increase in NPV during luteal
regression occurred in association with a decrease in luteal
area, progesterone and estradiol concentrations (4).
Decreased NPV during luteinization was attributed to
increased vascularization of luteal
tissue and a corresponding decreased tissue density (4). Increased NPV during luteolysis was attributed to decreased vascularization
and replacement of luteal tissue with fibrous
connective tissue, reflective of increased tissue density. Unfortunately, in
the present study, it was not possible to prove this theory because color
Doppler evaluation was not reported (4).
has not been
well-documented. CFFCs were attributed to the chance
occurrence of follicle rupture across a vascular component of the follicle
resulting in leakage of blood into the follicular lumen. Measurements of the luteal area, defined as the area between the external
border of the CL and the internal border of the CFFC, and luteal
numerical pixel value (NPV) were the main outcome measures of the study. Luteal area seems highly correlated with progesterone
concentrations during the interovulatory interval
(IOI). Luteal area and estradiol
concentrations, however, were not as strongly correlated. The regressing CL was
present in the follicular phase but it did not appear to be functional as
indicated by basal levels of serum progesterone and estradiol.
This study investigated also the quantitative changes
in luteal echotexture that
seems reflective of changes in the morphological and physiological status of the
CL in women. A decrease in luteal NPV occurred during
luteal development in association with an increase in
luteal area, progesterone and estradiol
concentrations, while the subsequent increase in NPV during luteal
regression occurred in association with a decrease in luteal
area, progesterone and estradiol concentrations (4).
Decreased NPV during luteinization was attributed to
increased vascularization of luteal
tissue and a corresponding decreased tissue density (4). Increased NPV during luteolysis was attributed to decreased vascularization
and replacement of luteal tissue with fibrous
connective tissue, reflective of increased tissue density. Unfortunately, in
the present study, it was not possible to prove this theory because color
Doppler evaluation was not reported (4).
|
|
|
|
|
|
|
|
|






The proximal thecal
arteriole, also called the helical arteriole of the CL, which can be easily
identified by power Doppler and which has a reproducible peak systolic velocity
(PSV) obtainable on pulsed Doppler imaging has been investigated (5,6).
Parsons (7), this vessel is responsible for feeding the CL and is characterized by high velocity flow and a higher PSV in comparison with luteal peripheral vessels. Recent data support the concept that blood flow into the CL reflects function, i.e. progesterone production. As suggested by Parsons (7), it has been shown that a simultaneous drop in arteriolar PSV and serum progesterone at 8 weeks of pregnancy that mirrors a similar effect in the fourth week of the menstrual cycle unless pregnancy intervenes (5).
REFERENCES
|
1. Nakata M, Selstam G, Olofsson J, Backstrom T.
Investigation of the human corpus luteum by ultrasonography: a proposed scheme for clinical
investigation. Ultrasound Obstet Gynecol 1992; 2: 190-196.
2. Backstrom T, Nakata M, Pierson RA. Ultrasonography
of normal and aberrant luteogenesis. In Imaging in Infertility and Reproductive
Endocrinology, Jaffe R , Pierson RA , Abramovwicz JS (eds). Lippincott-Raven:
3. Ottander U, Solensten NG, Bergh A, Olofsson JI. Intraovarian blood
flow measured with color Doppler ultrasonography
inversely correlates with vascular density in the human corpus luteum of the menstrual cycle. Fertil Steril 2004; 81: 154-159
4.
5. Guerriero S, Ajossa S, Lai MP, Risalvato A, Paoletti AM, Melis GB. Clinical applications of colour
Doppler energy imaging in the female reproductive tract and pregnancy. Hum Reprod Update
1999; 5: 515-529.
6. Guerriero S, Ajossa S, Melis GB. Imaging the human corpus luteum.
J Ultrasound Med 2001; 20: 1376-1377.
7. Parsons AK.
Imaging the human corpus luteum. J Ultrasound Med 2001; 20: 811-819.