|
POSSIBLE MECHANISMS OF INCREASED NUCHAL TRANSLUCENCY |
- Cardiac failure associated with abnormalities of the heart and great vessels.
- Septal or valvular defects (43%).
- Narrowing of the aortic isthmus and narrowing immediately above the aortic valve (86%) (1).
- Venous congestion in the head and neck.
- Constriction of the fetal body (amnion rupture sequence).
- Superior mediastinal compression (diaphragmatic hernia).
- Narrow thoracic cavity (skeletal dysplasia e.g. Thanatophoric dwarfism).
- Failure of lymphatic drainage due to abnormal or delayed development of the lymphatic system (2).
- Impaired fetal movements.
- Fetal neuromuscular disorders.
- Altered composition of subcutaneous connective tissue.
- Fetal anemia or hypoproteinemia.
|
DUCTUS VENOSUS BLOOD FLOW AND NUCHAL TRANSLUCENCY |
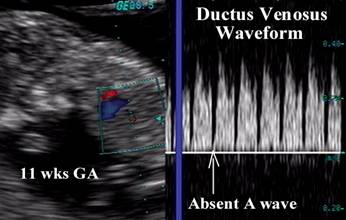
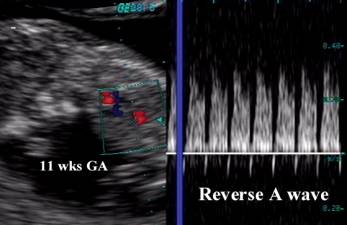
In addition to NT measurement, first-trimester ductus venosus (DV) flow studies have been identified as useful for aneuploidy screening. Forward biphasic pulsatile DV flow is normal, whereas reversed flow at the time of atrial contraction has been associated with aneuploidy and cardiac defects (3). Studies evaluating this association found between 59% and 93% of aneuploid fetuses had abnormal DV flow velocities, with the same finding present in only 3% to 21% of chromosomally normal fetuses (3-8).
Study of the DV flow velocity waveform following an NT ultrasound evaluation may be useful in modifying a patient's risk for aneuploidy. The use of this approach may be to improve the detection rate of NT ultrasound alone, or alternatively to reduce the false-positive rate.
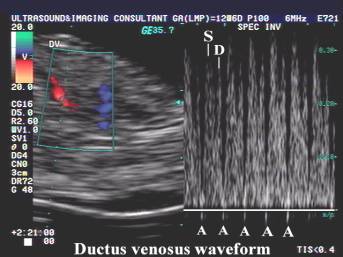
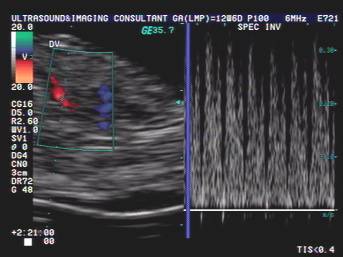
The ductus venosus is a unique shunt that carries well oxygenated blood from the umbilical vein directly into the cerebral and coronary circulation. It has a high pulsatile forward flow throughout the cardiac cycle, and appears to be useful in assessing cardiac function.
Link to the normal Ductus Venosus
In
situations of cardiac failure in the late second and third trimesters, with or
without cardiac defects, reversed flow during atrial contraction (A wave) may
be present. In the first trimester, this may be a normal finding prior to 15
weeks of gestation, however in the presence of increased nuchal translucency,
this may be due to cardiac dysfunction due to an underlying cardiac defect. It
has been suggested that there may be a temporary functional abnormality either
in the ventricles, aortic outflow tract or ductus itself. We have personally
demonstrated an increased frequency of left sided cardiac defects (hypoplastic
Down syndrome
–
Increased
nuchal translucency + reversed A wave in the ductus venosus |
|
|
|
|
|
|
|


|
|
Absent A wave |
|
|
Reverse A wave
|
Several drawbacks to DV flow studies should be considered:
· The DV vessel itself may be as small as 2 mm at 10 to 14 weeks and a typical Doppler gate size may vary from 0.5 to 2 mm in size.
· It can be difficult to obtain accurate flow velocity waveforms from such a tiny vessel without contamination of the waveform from neighboring blood vessels.
· If the Doppler gate is placed too proximally near the umbilical sinus, normal continuous venous flow from the umbilical vein may obscure the absence of flow during the atrial contraction in the DV.
· Placement of the Doppler gate too far distally, near the insertion of the DV into the inferior vena cava, may lead to the erroneous diagnosis of reversal of flow at the atrial contraction, because such reversal of flow is normal in the inferior vena cava.
· It is not sufficiently clear from published studies of NT and DV flow whether these two sonographic features are in fact completely independent of one another. If they are not then it may not be statistically valid to use one test to alter the risk assessment derived from the other. Based on these concerns, first-trimester DV Doppler flow studies may best be limited to predicting the prognosis of fetuses with normal chromosomes and increased NT (9).
REFERENCES |
- Hyett JA, Moscoso G, Papapanagiotou G et.al. Abnormalities of the heart and great vessels in chromosomally normal fetuses with increased nuchal translucency thickness at 11-13 weeks of gestation. Ultrasound Obstet Gynecol 1996;7:245-250.
- Greco P, Loverro G, Vimercati A et.al. Pathological significance of first trimester fetal nuchal edema. Prenat Diagn 1996;16:503-509.
- Matias
A, Gomes C, Flack N,
- Bilardo CM, Muller MA, Zikulnig L, Schipper M, Hecher K. Ductus venosus studies in fetuses at high risk for chromosomal or heart abnormalities: relationship with nuchal translucency measurement and fetal outcome. Ultrasound Obstet Gynecol 2001;17:288-94.
- Zoppi MA, Putzolu M, Ibba RM, Floris M, Monni G. First-trimester ductus venosus velocimetry in relation to nuchal translucency thickness and fetal karyotype. Fetal Diagn Ther 2002;17:52-7.
- Antolin E, Comas C, Torrents M, Munoz A, Figueras F, Echevarria M, et al. The role of ductus venosus blood flow assessment in screening for chromosomal abnormalities at 10–16 weeks of gestation. Ultrasound Obstet Gynecol 2001;17:295-300.
- Murta CG, Moron AF, Avila MA, Weiner CP. Application of ductus venosus Doppler velocimetry for the detection of fetal aneuploidy in the first trimester of pregnancy. Fetal Diagn Ther 2002;17:308-14.
- Mavrides E, Sairam S, Hollis B, Thilaganathan B. Screening for aneuploidy in the first trimester by assessment of blood flow in the ductus venosus. BJOG 2002;109:1015-9.
- Hecher K. Assessment of ductus venosus flow during the first and early second trimesters: what can we expect? Ultrasound Obstet Gynecol 2001;17:285-7.