|
RECOMMENDED VIEWS FOR
FETAL ECHOCARDIOGRAPHY |
WHY SCREEN FOR CARDIAC ANOMALIES? |
· Cardiac anomalies are the most common congenital malformations.
o Incidence of fetal cardiac malformations = 8:1000 live-births.
o Incidence of major congenital heart disease = 3-4:1000 live-births.
· Incidence of cardiac malformations are 6.5 times more common than chromosomal anomalies.
· Incidence of cardiac malformations are 4 times more common than neural tube defects.
· Most infants (up to 80%) with cardiac malformations are born to mothers with no known risk factors (low risk patient). There prenatal detection is dependent on sensitive prenatal screening protocols.
· Major congenital heart disease may be defined as complex structural malformations of the heart and great vessels that requires surgical or catheter intervention within the first 6 months to twelve months of life.
· 20-25% of neonatal deaths are attributable to congenital abnormalities (up to 50% of theses infants have cardiac disease).
· There is therefore convincing evidence that fetal echocardiography should be routinely included in every scan. Antenatal detection impacts: Further management; parental counseling (amniocentesis, outcome etc); planning obstetrical and neonatal care (especially in the presence of ductus dependent lesions).
We suggest that a routine fetal echocardiogram should employ five transverse (axial) images and two sagittal images.
TRANSVERSE (AXIAL) VIEWS |

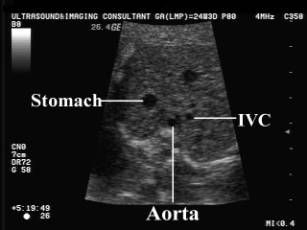
A1 Transverse (axial) view through the upper
abdomen.



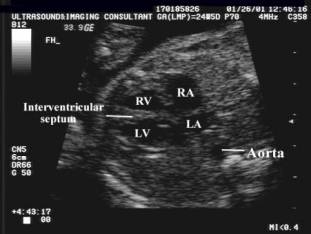
A2 Traditional four-chamber view of the heart
(apical and subcostal views).

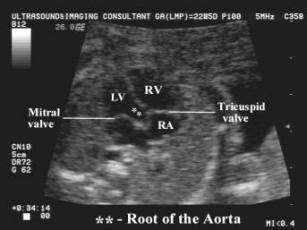
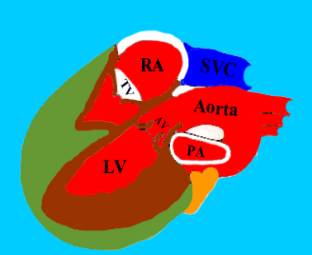
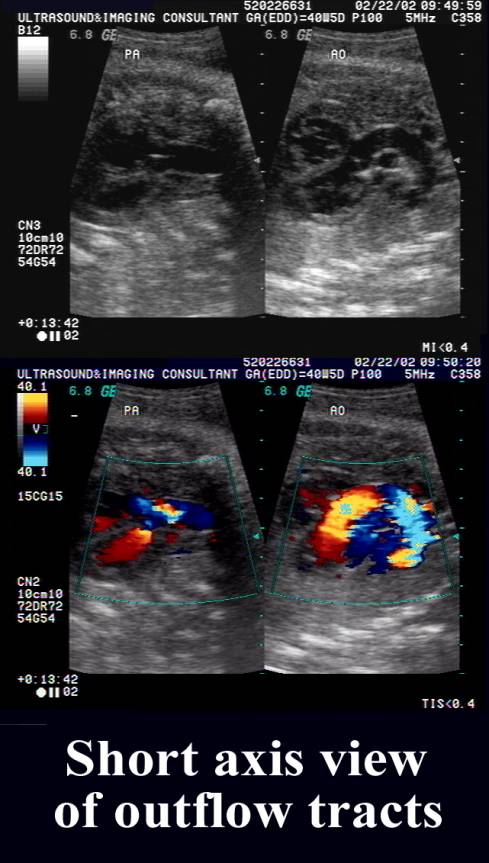
A3 Aortic and pulmonary outflow tracts.


A4 Pulmonary artery bifurcation.

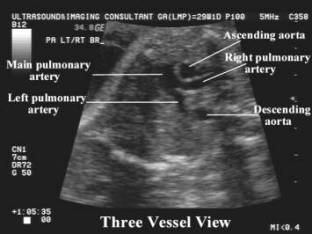

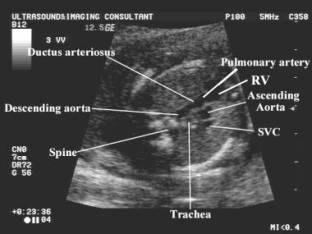
A5 Three-vessel view.

|
|
Video clip of the five axial views of the heart
|
|
|
|
|
|

SAGITTAL VIEWS |

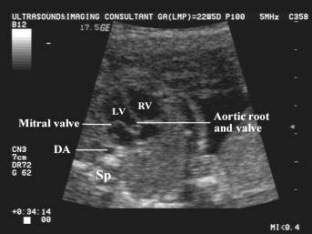
S1 Ductal arch.


S2 Aortic arch.



|
|
Video clip of
Aortic and Ductal Arches - Sagittal plane
|
|
|
|
|
|
